Does Dietitian Involvement During Pregnancy Improve Birth Outcomes? A Systematic Review
Publication: Canadian Journal of Dietetic Practice and Research
30 May 2023
Abstract
Maternal diet during pregnancy can have a significant impact on maternal and offspring health. As nutrition counselling is an important component of prenatal care, registered dietitians (RDs) are uniquely trained professionals who can provide personalized nutrition counselling customized to an individual’s sociocultural needs. The objective of this systematic review was to determine if RD involvement during pregnancy is associated with a lower prevalence of adverse birth outcomes in the United States and Canada. The review was conducted through a search of four databases: PubMed, CINAHL, Embase, and Web of Science. A total of 14 studies were identified. Women had a lower prevalence of low birth weight and preterm infants when RDs were involved during prenatal care. While RD involvement during pregnancy was not associated with macrosomia, more research is needed to assess its relationship with small for gestational age, large for gestational age, and infant mortality. Future research should also investigate the specific dietary advice provided by RDs and the extent and timing of their involvement throughout pregnancy to better understand the mechanisms surrounding nutrition counselling, in utero development, and health outcomes.
Résumé
L’alimentation de la mère pendant la grossesse peut avoir un impact important sur la santé de la mère et de l’enfant. Le counseling nutritionnel étant une composante importante des soins prénatals, les diététistes (RD), des professionnels possédant une formation unique, peuvent fournir des conseils nutritionnels personnalisés et adaptés aux besoins socioculturels de la personne. L’objectif de cette revue systématique était de déterminer si l’implication des RD pendant la grossesse est associée à une prévalence plus faible d’issues défavorables de la grossesse aux États-Unis et au Canada. La revue a été réalisée au moyen de recherches dans quatre bases de données : PubMed, CINAHL, Embase et Web of Science. Au total, 14 études canadiennes ont été ciblées. La prévalence de faible poids à la naissance et de prématurité était plus faible lorsque des RD s’étaient impliquées dans les soins prénatals. Bien que l’implication des RD pendant la grossesse n’ait pas été associée à la macrosomie, des recherches supplémentaires sont nécessaires pour évaluer sa relation avec un bébé petit par rapport à l’âge gestationnel, un bébé gros par rapport à l’âge gestationnel et la mortalité infantile. Les recherches futures devraient également porter sur les conseils nutritionnels fournis par les RD et sur l’étendue et le moment de leur implication pendant la grossesse afin de mieux comprendre les mécanismes entourant le counseling nutritionnel, le développement in utero et les résultats en matière de santé.
INTRODUCTION
Maternal diet during pregnancy can have a significant impact on maternal and offspring health [1]. While pregnancy outcomes can be affected by environmental, demographic, medical, behavioural, and socioeconomic factors [2], the importance of adequate weight gain, balanced meals, vitamin and mineral supplementation, alcohol and drug avoidance, and food safety cannot be overemphasized, as they are key factors associated with healthy pregnancies. As nutrition counselling is an important component of prenatal care, registered dietitians (RDs) are uniquely trained professionals who can provide nutrition counselling customized to an individual’s sociocultural needs.
In 2009, the Institute of Medicine (IOM) modified its 1990 guidelines for gestational weight gain, which considers prepregnancy body mass index (BMI) as an important predictor of birth weight [3]. Gestational weight gain below the recommended range for prepregnancy BMI increases the likelihood of having a low birth weight infant, whereas excessive gestational weight gain is associated with a higher risk for fetal macrosomia [4, 5]. Although RDs are not required members of prenatal health care teams in Canada and the United States, and studies supporting RDs’ roles have not been comprehensively evaluated [6], referrals to RDs are common for high-risk pregnancies, whereas resources remain limited for low-risk pregnancies [7]. Yet, randomized controlled trials (RCTs) have shown that RD involvement during pregnancy is associated with improved dietary intake and adherence to gestational weight guidelines for both low-risk and high-risk pregnancies [8–11].
Given that prenatal diets are a modifiable risk factor for gestational weight gain and adverse birth outcomes, dietetic counselling may correlate with more optimal birth outcomes. However, existing studies on the association between RD involvement and birth outcomes have been inconsistent, with some studies showing positive effects and others having null findings. Vesco et al. found that an intensive dietary intervention initiated by RDs is associated with a lower prevalence of large-for-gestational-age infants (9%) compared to groups receiving only one-time dietary advice (26%) [12]. Crowther et al. found a significantly lower incidence of large for gestational age (13%) and macrosomia (10%) as a result of RD involvement compared to a control group (22% and 21%) [13]. Other studies have found no effect of RD involvement during pregnancy on infant outcomes [14, 15]. Low birth weight (LBW), preterm birth (PTB), small for gestational age (SGA), and mortality are the most common outcomes evaluated in the literature, and there have been recommendations for more research on large for gestational age (LGA) and macrosomia [16].
The objective of this systematic review was to determine if RD involvement during pregnancy is associated with a lower prevalence of LBW, PTB, SGA, LGA, macrosomia, and infant mortality. This is the first systematic review to assess these relationships.
METHODS
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [17]. A protocol was registered with The Open Science Framework (https://osf.io/k5nup) on February 16 2022. The PICOS framework guided the search strategy: Population (pregnant individuals); Intervention/Exposure (direct involvement by an RD or as part of a multidisciplinary team during pregnancy); Comparator (no RD involvement during pregnancy or standard care by an RD); Outcomes (LBW, SGA, LGA, macrosomia, PTB, infant mortality); Study Design (observational and experimental studies). Using a narrative analysis, the association between RD involvement during pregnancy and birth outcomes was assessed, summarized, and synthesized for all eligible studies.
Search strategy
Comprehensive literature searches of PubMed (1966–2021), CINAHL (1937–2021), Embase (1947–2021), and Web of Science (1970–2021) were conducted independently on December 18 2021 by two authors (WL and MH). A search strategy was developed using the key search terms in Supplementary File A1. Search string, MeSH terms, and subject headings were then created for each database. The search strategy was developed by the authors and a health sciences librarian at Brescia University College. Search results from the four databases were imported into Covidence (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia. 2022), and duplicates were removed. Covidence was used to screen titles, abstracts, and full texts. Reference lists of retrieved articles were assessed to identify additional studies not obtained in the original search.
Study eligibility criteria
Studies needed to be original research, written in English, conducted in Canada and (or) the United States, and include pregnant individuals. The search was limited to the two countries to ensure consistency in the legal practice of RDs. Each study should have observed at least one of the six birth outcomes: LBW (<2500g), SGA (birth weight <10th percentile for gestational age or infants smaller in size than normal for their gestational age) [18, 19], LGA (a birth weight >90th percentile) [20], macrosomia (birth weight >4000g) [21], PTB (<37 weeks’ gestation), and infant mortality (death of the fetus or infant death following a live birth; i.e., stillbirth, neonatal death, and perinatal death). Eligible studies must have had direct involvement from an RD or those with equivalent legal titles (Supplementary File B1). Direct involvement was defined as nutrition practice (i.e., nutrition interventions, dietary changes/plan, nutrition counselling, or medical nutrition therapy) by an RD alone or as a part of a multidisciplinary team. Reviews, editorials, letters, and grey literature were excluded. There were no restrictions on study design or publication dates.
Title, abstract, and full-text screening were conducted independently by two authors (WL and MH), with conflicts resolved by consensus or adjudication with the senior author (JAS).
Data extraction
A standardized coding guide was developed using Microsoft Excel (Microsoft Corporation, Redmond, Washington, USA, 2019). Information included were publication year, author name(s), objectives, sample characteristics (e.g., health status, maternal age, race/ethnicity, socioeconomic status), geographic location, sample size, study design, types of RD involvement, key findings, and study limitations. Two authors (WL and MH) independently extracted data and collectively resolved discrepancies. The senior author (JAS) adjudicated any unresolved discrepancies.
Study quality assessment
The methodological quality of studies was assessed by two independent authors (WL and MH) using the JBI critical appraisal tool [22, 23]. This tool determined the risk of bias through a customized checklist created for each study. A specific JBI checklist was used for cross-sectional studies, case-control studies, cohort studies, and RCTs [22, 23]. The checklist consisted of four possible answers: “yes,” “no,” “unclear,” and “not applicable.” Answers that were “not applicable” were excluded from the final count towards determining the overall quality rating of each paper. The quality rating of each study was determined using a three-range scale (≥ 80% “yes” is good; 60-79% “yes” is fair; ≤ 59% “yes” is poor). The three-range scale and its ratings closely align with other studies using the JBI [24, 25]. Checklist questions and a summary of the assessment can be found in Supplementary Tables 1–41.
RESULTS
Description of studies
The search strategy identified 310 studies, 114 were removed as duplicates, and 196 required screening. From the 196 articles, 188 did not meet inclusion criteria. Six additional articles were retrieved from reference lists screened. Therefore, 14 studies were included in this systematic review (Figure 1).
Figure 1.
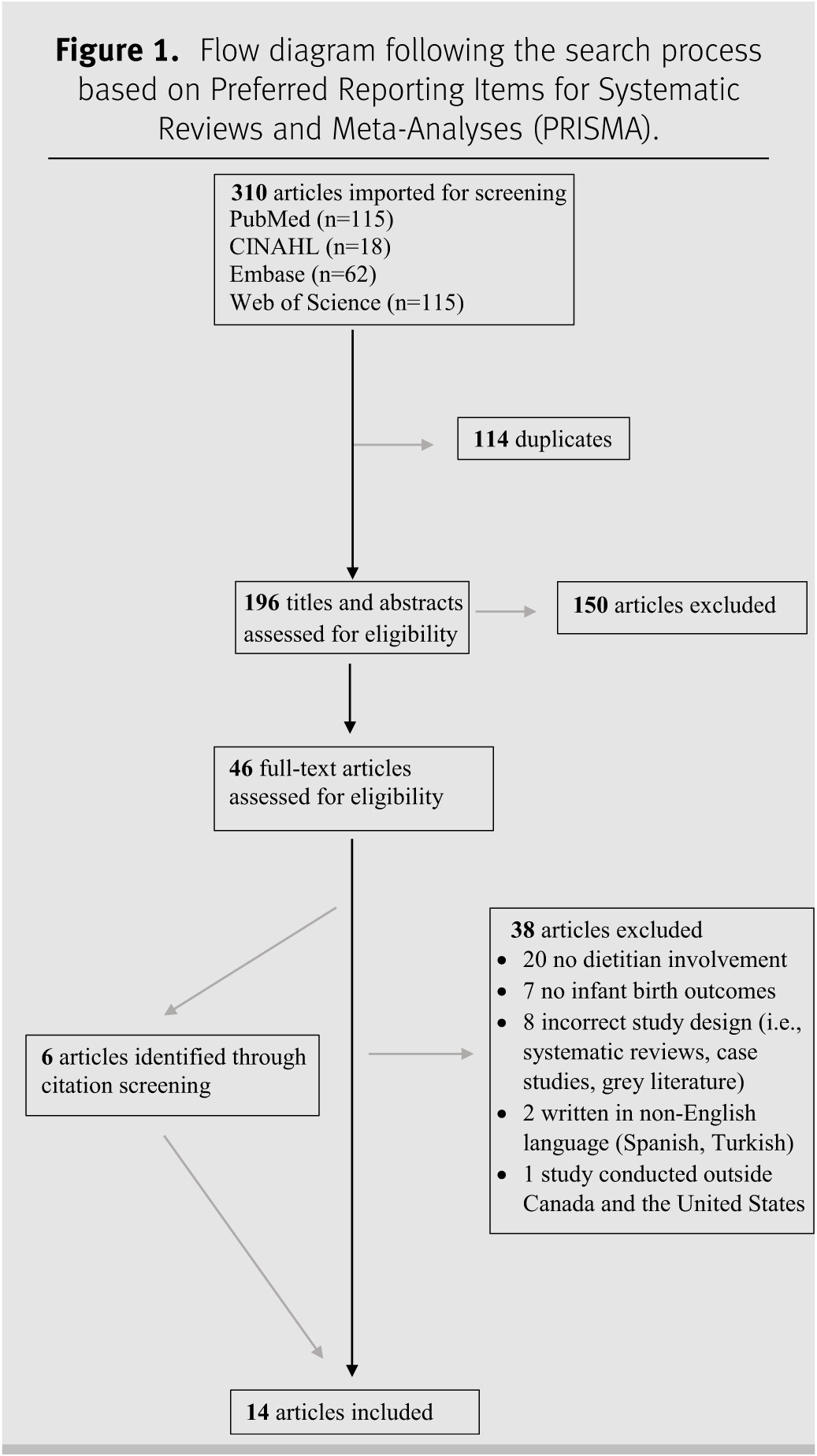
Thirteen studies were conducted in the United States, and 1 study was from Canada. The publication years ranged from 1989 to 2018. Study designs consisted of 2 cross-sectional studies, 2 case-control studies, 3 retrospective cohort studies, 5 RCTs, 1 implementation trial, and 1 pilot study. Low birth weight was examined in 7 studies, SGA in 3 studies, LGA in 4 studies, macrosomia in 6 studies, PTB in 9 studies, and infant mortality in 2 studies. The average age of pregnant women was 29.3 years among 9 studies, with 1 study specifying the common age as 20 to 24 years [26] and another study specifying the median age as 26.8 years in its study group and 37.3 years in its control group [27]. Three studies did not report maternal age [28–30]. Seven studies described participants’ gestational age. Most women entered the studies before the 28th week of gestation, although participants in 3 studies joined before 16 weeks of gestation [12, 28, 31]. Sample sizes ranged from 87 to 2,377 participants. Eleven of the 14 studies included diverse ethnic groups. Registered dietitian involvement during pregnancy included nutrition care, education, and counselling. A description of the studies (e.g., study design, sample characteristics, type of RD involvement) can be found in Table 1.
Table 1.
Note: a Mean age at the onset of pregnancy for the sample, similar age distribution in all three groups. N.B.: CDAPP = California Diabetes and Pregnancy Program; DASH = Dietary Approaches to Stopping Hypertension; GDM = Gestational Diabetes Mellitus; GWG = gestational weight gain; LGA = large for gestational age; LBW = low birth weight; PTB = preterm birth; PRN = “pro re nata”/as needed; RD = registered dietitians; RCTs = randomized controlled trials; SGA = small for gestational age; IOM = Institute of Medicine; US = United States.
*Included pregnancy-related risks of being overweight or obese, a review of the IOM gestational weight gain recommendation based on participants’ BMIs, information on basic nutritional needs, healthy eating, and safe exercise during pregnancy. **Included dietary assessment, individualized meal plans, and additional counselling topics; twice a month throughout pregnancy. ***Total participants.
Low birth weight
Four of the 5 studies that compared RD involvement to no RD involvement found a lower prevalence of LBW in groups with RD involvement [26, 31–33]. When comparing standard RD care to advanced RD care, an RCT [34] found no difference between groups receiving standard nutrition counselling (control) compared to advanced nutrition care (intervention), although very few patients had LBW overall. For example, among women identified as normal weight at the first prenatal visit, 5/92 women had a LBW infant in the control group versus 4/90 in the intervention group. Similarly, only 4/86 overweight women had a LBW infant in the control group compared to 5/81 in the intervention group. One study found that 9.7% of all participants had a LBW infant, although LBW was reduced to 6.7% among women with adequate gestational weight gain, compared to 17.2% among those with inadequate weight gain (p < 0.001) [30]. In an implementation trial for clinical practice guidelines [35], both the intervention and control groups included RDs. Registered dietitians in the intervention group (n = 130) provided prenatal care as described in nutrition practice guidelines for gestational diabetes mellitus (GDM), whereas RDs in the control group (n = 85) provided usual prenatal care. No statistically significant difference in LBW was found between the nutrition practice guidelines group and the usual care group (2.4% vs. 8.4%, respectively, p = 0.27) [35].
Small for gestational age
In an RCT by Peccei et al. assessing the effect of a culturally appropriate nutritional intervention delivered to overweight and obese patients in a community health setting, there was no significant difference in SGA prevalence between the RD involvement intervention group and the control group (6.1% vs. 3.3%; odds ratio [OR] = 1.9, 95% confidence interval [CI]: 0.5–7.1) [28]. In the RCT by Vesco et al., where the intervention group received individualized nutrition counselling and the control group received one-time dietary advice, no significant difference in SGA was found between the intervention and control group (5% vs. 7%; OR = 0.76, 95% CI: 0.11−4.76) [12]. In Artal et al.’s RCT, both groups received medical nutrition therapy (MNT) administrated by RDs, and there was no difference in the rate of SGA in the group receiving MNT and exercise (2/39; 5.9%) to those receiving the diet intervention alone (1/57; 2.2%) [36].
Large for gestational age
Fassett et al. found no significant difference in LGA between the RD involvement group and the non-RD involvement group (14% vs. 14%; p = 0.94) [37]. Peccei et al. examined LGA among all participants and separately among obese participants [28]. The intervention group, which involved intensive prenatal nutrition counselling by an RD, was not significantly different from the control group (6% vs. 13%; OR = 0.4, 95% CI: 0.2-1.0; p = 0.058) for LGA. Among obese participants however, those in the intervention group had 70% lower odds of LGA infants than in the control group, and the difference was statistically significant (7% vs. 17%; OR = 0.3, 95% CI: 0.1–0.99; p = 0.048) [28]. An RCT by Vesco et al. also found a significantly lower prevalence of LGA in the intervention group than the control group (9% vs. 26%; OR = 0.28, 95% CI: 0.09–0.84) [12]. In the Artal et al. RCT, both groups received a diet intervention, but there was no significant different in LGA between the group receiving MNT alone (7/57) and the group receiving an additional exercise intervention (4/39) (p = 0.64) [36].
Macrosomia
The retrospective case-control study by Fassett et al. revealed no difference in macrosomia between the RD involvement group and the non-RD involvement comparator (14% vs. 14%; p = 0.94) [37]. The pilot study by Weiderman et al. also found no significant difference between groups with and without RD involvement (p = 0.40) [29]. Phelan et al. found that, among those with a prepregnancy BMI indicating normal weight, 3/92 birthed children with fetal macrosomia in the standard nutrition care group compared to 6/90 in the intensive nutrition care group [34]. For women with a prepregnancy BMI indicating overweight, the rates of macrosomia were 14/86 (16.3%) and 14/81 (17.3%) for the standard and intensive nutrition care groups, respectively. In studies by Reader et al. [35], Vesco et al. [12], and Thornton et al. [27], there were no statistically significant differences in macrosomia in the control groups receiving basic nutrition care (i.e., nutrition counselling) and the groups receiving extensive nutrition care (i.e., dietary advice, weight gain discussions, dietitian follow-ups).
Preterm birth
Among 5 studies examining PTB that compared groups with RD involvement to those without RD involvement, 4 studies found a lower prevalence of PTB in groups with RD involvement [26, 31–33], with 2 studies indicating a significant difference [31, 32]. One study found no significant difference between groups [38]. Among the remaining 4 studies, all participants received nutrition care by RDs, with 1 study indicating a lower prevalence of PTB in groups receiving extensive nutrition care [34], and 3 studies finding no significant differences in PTB between groups receiving standard and in-depth nutrition care [12, 27, 35].
Infant mortality
DISCUSSION
Main findings
This systematic review demonstrates that pregnant individuals have a lower prevalence of LBW infants when RDs are involved during prenatal care. This is an important finding because LBW increases the risk for infant mortality, poor cognitive development, respiratory distress, and asthma during childhood, and cardiovascular disease, type 2 diabetes, and hypertension during adulthood [2]. While the etiology of LBW is multifactorial [39, 40], poor maternal nutrition is a major contributing factor [41, 42]. Two of the 4 studies which found a lower prevalence of LBW with RD involvement compared to no involvement were of good quality, 1 was fair quality, and 1 was poor quality. RD involvement was also associated with a lower prevalence of PTB, particularly when RD involvement was compared to no involvement (4/5 studies). Furthermore, while RD involvement during pregnancy was not associated with macrosomia, more research is needed to elucidate its correlation with SGA, LGA, and infant mortality. All 3 studies that assessed SGA as an outcome were not of good methodological quality. Additionally, 2/4 studies found a reduction in LGA infants with RD involvement compared to no involvement, and only 2 studies assessed infant mortality, both of which found a lower rate of mortality with RD involvement.
Interpretation
Although this systematic review investigates the association between RD involvement during pregnancy and birth outcomes in Canada and the United States, our findings are fairly consistent with studies from other countries. In a quasi-experimental design from Mexico City, Perichart-Perera et al. [43] examined the relationship between dietitian-initiated MNT (i.e., counselling, education, and capillary glucose monitoring) and birth outcomes. Among women with GDM, the MNT group were significantly less likely to have a LBW infant than the control group (5.1 % vs 20.5%, p = 0.03), although there were no differences in LBW between groups among women with type 2 diabetes. The study found no significant differences in rates of prematurity and macrosomia between the two groups. In an RCT from Australia examining whether treatment of women with GDM reduced the risk of perinatal complications, Crowther et al. [13] found that the intervention group (n = 506, receiving dietary advice from an RD, blood glucose monitoring, insulin therapy) was significantly less likely than the routine-care group (n = 524) to have an LGA (13% vs. 22%, p < 0.001) or fetal macrosomia (10% vs 21%, p < 0.001) outcome, although SGA was similar between the two groups. Noteworthy is that the current review includes various population types, such as twin pregnancies, adolescent pregnancies, obese pregnant women, and women diagnosed with GDM, all of which increase the risk for adverse birth outcomes [44–47]. It is plausible that pregnant individuals may have received different nutrition care from RDs depending on their health concerns and conditions, adding to greater heterogeneity in the exposure.
Strengths and limitations
This systematic review provides a comprehensive assessment of the association between RD involvement during pregnancy and birth outcomes in Canada and the United States. Given that many prenatal health care providers report insufficient education and training in nutrition [48, 49], and that dietitians are regulated health professionals who undergo rigorous training, RD advice to pregnant individuals (e.g., recommended foods and those to avoid) may enhance maternal health and fetal development, if the advice is followed. However, there are some limitations to consider when interpreting these findings. First, there was limited sociodemographic information reported in most studies with respect to race, ethnicity, and socioeconomic status. This is unfortunate because research shows that pregnant women who are non-Hispanic Black, Hispanic, and those with low educational attainment have poorer diet quality than those who are non-Hispanic Whites [50]. Future research should address the extent to which RD involvement during pregnancy can attenuate disparities in birth outcomes by factors such as socioeconomic status, race, and ethnicity. Second, several studies had inadequate statistical power to detect clinically meaningful results in birth outcomes. Underpowered studies are problematic because they increase the risk of a type II error/false negative [51]. While underpowered studies can sometimes be mitigated by pooling the data when conducting a meta-analysis, the heterogeneity would have been very large between the included studies since the definition of RD involvement varied considerably. Future interventions that involve RDs during pregnancy need to accurately specify the content and frequency of their involvement.
RELEVANCE TO PRACTICE
Although more research is warranted on the relationship between RD involvement and adverse birth outcomes, our systematic review suggests that RD involvement during prenatal care is associated with a lower prevalence of LBW and PTB, both of which increase the risk for infant morbidity and mortality, and the development of chronic health conditions in adulthood. These findings are important and indicate a need for greater advocacy from other health care professionals with regard to the importance of dietitian services during pregnancy. Future research should investigate the specific dietary advice provided by RDs and the extent and timing of their involvement throughout pregnancy.
Financial support: The authors declare that no external financial support was given for purposes of this manuscript.
Conflict of interest: The authors declare they have no competing interests.
Footnote
1
Supplementary data are available with the article at Supplementary Material.
REFERENCES
1
Procter SB and Campbell CG. Position of the academy of nutrition and dietetics: nutrition and lifestyle for a healthy pregnancy outcome. J Acad Nutr Diet. 2014 Jul;114(7):1099–1103.
2
Campbell EE and Seabrook JA. The influence of socioeconomic status on adverse birth outcomes. Can J Midwifery Res Pract. 2016;15(2):11–20.
3
Rasmussen KM, Yaktine AL, editors. Weight gain during pregnancy: reexamining the guidelines. Washington (DC)2009.
4
Liang CC, Chao M, Chang SD, and Chiu SY. Pregnancy weight gain may affect perinatal outcomes, quality of life during pregnancy, and child-bearing expenses: an observational cohort study. Arch Gynecol Obstet. 2021 Sep;304(3):599–608.
5
Campbell EE, Dworatzek PD, Penava D, de Vrijer B, Gilliland J, Matthews JI, et al. Factors that influence excessive gestational weight gain: moving beyond assessment and counselling. J Matern Fetal Neonatal Med. 2016 Nov;29(21):3527–31.
6
Pari-Keener M, Gallo S, Stahnke B, McDermid JM, Al-Nimr RI, Moreschi JM, et al. Maternal and infant health outcomes associated with medical nutrition therapy by registered dietitian nutritionists in pregnant women with malnutrition: an evidence analysis center systematic review. J Acad Nutr Diet. 2020 Oct;120(10):1730–1744.
7
Forbes L, Baarda J, Mayan M, and Bell RC. Qualitative assessment of key messages about nutrition and weight gain in pregnancy in printed educational materials in Alberta. Can J Diet Pract Res. 2017 Dec 1;78(4):182–186.
8
Hui A, Back L, Ludwig S, Gardiner P, Sevenhuysen G, Dean H, et al. Lifestyle intervention on diet and exercise reduced excessive gestational weight gain in pregnant women under a randomised controlled trial. BJOG. 2012 Jan;119(1):70–77.
9
Buckingham-Schutt LM, Ellingson LD, Vazou S, and Campbell CG. The Behavioral Wellness in Pregnancy study: a randomized controlled trial of a multi-component intervention to promote appropriate weight gain. Am J Clin Nutr. 2019 Apr 1;109(4):1071–1079.
10
Yang J, Wang M, Tobias DK, Rich-Edwards JW, Darling AM, Abioye AI, et al. Dietary diversity and diet quality with gestational weight gain and adverse birth outcomes, results from a prospective pregnancy cohort study in urban Tanzania. Matern Child Nutr. 2022 Apr;18(2):e13300.
11
Accortt EE, Cheadle AC, and Dunkel Schetter C. Prenatal depression and adverse birth outcomes: an updated systematic review. Matern Child Health J. 2015 Jun;19(6):1306–1337.
12
Vesco KK, Karanja N, King JC, Gillman MW, Leo MC, Perrin N, et al. Efficacy of a group-based dietary intervention for limiting gestational weight gain among obese women: a randomized trial. Obesity (Silver Spring). 2014 Sep;22(9):1989–1996.
13
Crowther CA, Hiller JE, Moss JR, McPhee AJ, Jeffries WS, Robinson JS, et al. Effect of treatment of gestational diabetes mellitus on pregnancy outcomes. N Engl J Med. 2005 Jun 16;352(24):2477–2486.
14
Koivusalo SB, Rono K, Klemetti MM, Roine RP, Lindstrom J, Erkkola M, et al. Gestational diabetes mellitus can be prevented by lifestyle intervention: the Finnish gestational diabetes prevention study (RADIEL): a randomized controlled trial. Diabetes Care. 2016 Jan;39(1):24–30.
15
Dodd JM, Deussen AR, and Louise J. A randomised trial to optimise gestational weight gain and improve maternal and infant health outcomes through antenatal dietary, lifestyle and exercise advice: the OPTIMISE randomised trial. Nutrients. 2019 Dec 2;11(12).
16
Frank CE, Speechley KN, Macnab JJ, and Campbell MK. Infants born large for gestational age and developmental attainment in early childhood. Int J Pediatr. 2018;2018:1.
17
Moher D, Liberati A, Tetzlaff J, Altman DG, and Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009 Jul 21;6(7):e1000097.
18
Osuchukwu OO, Reed DJ. Small for gestational age. BTI - StatPearls.
19
Schlaudecker EP, Munoz FM, Bardají A, Boghossian NS, Khalil A, Mousa H, et al. Small for gestational age: case definition & guidelines for data collection, analysis, and presentation of maternal immunisation safety data. Vaccine. 2017 2017/12/04/;35(48, Part A):6518–28.
20
Weissmann-Brenner A, Simchen MJ, Zilberberg E, Kalter A, Weisz B, Achiron R, et al. Maternal and neonatal outcomes of large for gestational age pregnancies. Acta Obstetricia et Gynecologica Scandinavica. 2012;91(7):844–849.
21
Kc K, Shakya S, and Zhang H. Gestational diabetes mellitus and macrosomia: a literature review. Ann Nutr Metab. 2015;66 66:14–20.
22
Tufanaru CMZ, Aromataris E, Campbell J, Hopp L. Chapter 3: Systematic reviews of effectiveness. 2020 [cited 2022 June 16]; Available from: https://synthesismanual.jbi.global.
23
Moola SMZ, Tufanaru C, Aromataris E, Sears K, Sfetcu R, Currie M, Qureshi R, Mattis P, Lisy K, Mu P-F. Chapter 7: Systematic reviews of etiology and risk. 2020 [cited 2022 June 16]; Available from: https://synthesismanual.jbi.global.
24
Kanda P, Gupta A, Gottlieb C, Karanjia R, Coupland SG, and Bal MS. Pathophysiology of central serous chorioretinopathy: a literature review with quality assessment. Eye (Lond). 2022 May;36(5):941–962.
25
Zhang Q, Mu MC, He Y, Cai ZL, and Li ZC. Burnout in emergency medicine physicians: A meta-analysis and systematic review. Medicine (Baltimore). 2020 Aug 7;99(32):e21462.
26
Bahry VJ, Fullerton JT, and Lops VR. Provision of comprehensive perinatal services through rural outreach: A model program. J Rural Health. 1989;5(4):387–396.
27
Thornton YS, Smarkola C, Kopacz SM, and Ishoof SB. Perinatal outcomes in nutritionally monitored obese pregnant women: a randomized clinical trial. J Natl Med Assoc. 2009 Jun;101(6):569–77.
28
Peccei A, Blake-Lamb T, Rahilly D, Hatoum I, and Bryant A. Intensive prenatal nutrition counseling in a community health setting a randomized controlled trial. Obstet Gynecol. 2017;130(2):423–432.
29
Weiderman WC, Marcuz L, and Platt LD. Gestational diabetes: a triage model of care for rural perinatal providers. Am J Obstet Gynecol. 1996;174(6):1719–1724.
30
Ricketts SA, Murray EK, and Schwalberg R. Reducing low birthweight by resolving risks: results from Colorado’s prenatal plus program. Am J Public Health. 2005;95(11):1952–1957.
31
Luke B, Brown MB, Misiunas R, Anderson E, Nugent C, van de Ven C, et al. Specialized prenatal care and maternal and infant outcomes in twin pregnancy. Am J Obstet Gynecol. 2003 Oct;189(4):934–938.
32
Morris DL, Berenson AB, Lawson J, and Wiemann CM. Comparison of adolescent pregnancy outcomes by prenatal care source. J Reprod Med. 1993;38(5):375–80.
33
Dubois S, Dougherty C, Duquette MP, Hanley JA, and Moutquin JM. Twin pregnancy: the impact of the Higgins Nutrition Intervention Program on maternal and neonatal outcomes. Am J Clin Nutr. 1991 Jun;53(6):1397–1403.
34
Phelan S, Phipps MG, Abrams B, Darroch F, Schaffner A, and Wing RR. Randomized trial of a behavioral intervention to prevent excessive gestational weight gain: the Fit for Delivery Study. Am J Clin Nutr. 2011 Apr;93(4):772–779.
35
Reader D, Splett P, and Gunderson EP. Impact of gestational diabetes mellitus nutrition practice guidelines implemented by registered dietitians on pregnancy outcomes. J Am Diet Assoc. 2006;106(9):1426–1433.
36
Artal R, Catanzaro RB, Gavard JA, Mostello DJ, and Friganza JC. A lifestyle intervention of weight-gain restriction: diet and exercise in obese women with gestational diabetes mellitus. Appl Physiol Nutr Metab. 2007 Jun;32(3):596–601.
37
Fassett MJ, Dhillon SHK, and Williams TR. Effects on perinatal outcome of treating women with 1 elevated glucose tolerance test value. Am J Obstet Gynecol. 2007;196(6):597.e1–597.e4; discussion.e4.
38
Gandhi M, Hosseinzadeh P, Salmanian B, Moaddab A, Golabbakhsh H, Clark SL, et al. Dietary consultation impact on weight gain in twin pregnancies. J Reprod Med. 2018;63(7–8):347–51.
39
Seabrook JA, Smith A, Clark AF, and Gilliland JA. Geospatial analyses of adverse birth outcomes in Southwestern Ontario: examining the impact of environmental factors. Environ Res. 2019 May;172:18–26.
40
Mayer C and Joseph KS. Fetal growth: a review of terms, concepts and issues relevant to obstetrics. Ultrasound Obstet Gynecol. 2013 Feb;41(2):136–145.
41
da Silva Lopes K, Ota E, Shakya P, Dagvadorj A, Balogun OO, Pena-Rosas JP, et al. Effects of nutrition interventions during pregnancy on low birth weight: an overview of systematic reviews. BMJ Glob Health. 2017;2(3):e000389.
42
Cetin I, Mando C, and Calabrese S. Maternal predictors of intrauterine growth restriction. Curr Opin Clin Nutr Metab Care. 2013 May;16(3):310–319.
43
Perichart-Perera O, Balas-Nakash M, Parra-Covarrubias A, Rodriguez-Cano A, Ramirez-Torres A, Ortega-Gonzalez C, et al. A medical nutrition therapy program improves perinatal outcomes in Mexican pregnant women with gestational diabetes and type 2 diabetes mellitus. Diabetes Educ. 2009 Nov-Dec;35(6):1004–1013.
44
Goodnight W and Newman R, Society of Maternal-Fetal M. Optimal nutrition for improved twin pregnancy outcome. Obstet Gynecol. 2009 Nov;114(5):1121–1134.
45
DeMarco N, Twynstra J, Ospina MB, Darrington M, Whippey C, and Seabrook JA. Prevalence of low birth weight, premature birth, and stillbirth among pregnant adolescents in Canada: a systematic review and meta-analysis. J Pediatr Adolesc Gynecol. 2021 Aug;34(4):530–537.
46
McDonald SD, Han Z, Mulla S, Beyene J, and Knowledge Synthesis G. Overweight and obesity in mothers and risk of preterm birth and low birth weight infants: systematic review and meta-analyses. BMJ. 2010 Jul 20;341:c3428.
47
Sweeting AN, Ross GP, Hyett J, Molyneaux L, Constantino M, Harding AJ, et al. Gestational diabetes mellitus in early pregnancy: evidence for poor pregnancy outcomes despite treatment. Diabetes Care. 2016 Jan;39(1):75–81.
48
Lee A, Newton M, Radcliffe J, and Belski R. Pregnancy nutrition knowledge and experiences of pregnant women and antenatal care clinicians: A mixed methods approach. Women Birth. 2018 Aug;31(4):269–277.
49
Wennberg AL, Hamberg K, and Hornsten A. Midwives’ strategies in challenging dietary and weight counselling situations. Sex Reprod Healthc. 2014 Oct;5(3):107–112.
50
Bodnar LM, Simhan HN, Parker CB, Meier H, Mercer BM, Grobman WA, et al. Racial or ethnic and socioeconomic inequalities in adherence to national dietary guidance in a large cohort of US pregnant women. J Acad Nutr Diet. 2017 Jun;117(6):867–877.e3 e3.
51
Schaafsma H, Laasanen H, Twynstra J, and Seabrook JA. A review of statistical reporting in dietetics research (2010-2019): how is a Canadian journal doing? Can J Diet Pract Res. 2021 Jun 1;82(2):59–67.
Supplementary Material
File (cjdpr-2023-014suppla.docx)
- Download
- 25.08 KB
Information & Authors
Information
Published In

Canadian Journal of Dietetic Practice and Research
Volume 85 • Number 1 • March 2024
Pages: 32 - 44
Editor: Naomi Cahill
History
Version of record online: 30 May 2023
Copyright
© 2023.
Key Words
Mots-clés
Authors
Metrics & Citations
Metrics
Other Metrics
Citations
Cite As
MadehaHanifiMScFN(c), WenjunLiuMScFN(c), JasnaTwynstraPhD, and Jamie A.SeabrookPhD. 2024. Does Dietitian Involvement During Pregnancy Improve Birth Outcomes? A Systematic Review. Canadian Journal of Dietetic Practice and Research.
85(1): 32-44. https://doi.org/10.3148/cjdpr-2023-014
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
Cited by
1. Celebrating the Impact and Contribution of Dietitians
View Options
View options
Get Access
Login options
Check if you access through your login credentials or your institution to get full access on this article.
Subscribe
Click on the button below to subscribe to Canadian Journal of Dietetic Practice and Research