Exploring the Social Determinants of Health in Nutrition Care for South Asian Communities: A Narrative Review
Publication: Canadian Journal of Dietetic Practice and Research
17 January 2025
Abstract
The South Asian (SA) diasporic communities in Canada experience a greater burden of diabetes and cardiovascular disease (CVD) compared to white populations. Nutrition interventions often focus on individual behaviours and fail to consider that the social determinants of health (SDH) have a greater impact on chronic disease risk. A narrative review was conducted to identify the SDH in nutrition care interventions for the SA diaspora in Canada. The final analysis included fourteen articles from which SDH were identified and categorized based on the Social Ecological Model (SEM). The study analysis yielded the following needs in dietetic practice based on the SEM: (1) intrapersonal – need for language appropriate services, and representation of cultural foods and non-Western health perspectives in dietary guidelines, (2) interpersonal – understanding family and friends as social supports, (3) community – incorporating peer and community leader influences, (4) institution – importance of faith-based locations as community hubs, and client workplaces as a barrier to attending appointments, and (5) policy – advocacy for transportation and childcare access, adequate and secure income, and equitable care. These findings urge dietitians to move beyond cultural awareness, sensitivity, and competence to practicing cultural safety and humility in their practice, which is integral to providing equitable care.
Résumé
Les communautés diasporiques sud-asiatiques (SA) du Canada sont plus touchées par le diabète et les maladies cardiovasculaires (MCV) que les populations blanches. Les interventions nutritionnelles sont souvent axées sur les comportements individuels et ne tiennent pas compte du fait que les déterminants sociaux de la santé (DSS) ont un plus grand impact sur le risque de maladies chroniques. Une revue narrative a été menée afin d’identifier les DSS dans des interventions de soins nutritionnels destinées à la diaspora SA au Canada. L’analyse finale incluait quatorze articles où des DSS ont été identifiés et catégorisés sur la base du modèle socioécologique (MSE). L’analyse issue de l’étude a mis en lumière les besoins suivants dans la pratique de la diététique basée sur le MSE : (1) intrapersonnels – besoin de services linguistiquement adaptés et d’une représentation des aliments culturels et des perspectives de santé non occidentales dans les directives nutritionnelles, (2) interpersonnels – compréhension que la famille et les amis sont des soutiens sociaux, (3) communauté – intégration de l’influence des pairs et des leaders communautaires, (4) établissement – importance des lieux confessionnels en tant que carrefours pour les communautés, et des lieux de travail des clients en tant qu’obstacle à la participation aux rendez-vous, et (5) politiques – plaidoyer pour l’accès au transport et à la garde d’enfants, à un revenu adéquat et fixe, et à des soins équitables. Ces résultats révèlent que les diététistes doivent aller au-delà de la conscience, de la sensibilité et de la compétence culturelles et intégrer dans leur pratique la sécurisation culturelle et l’humilité, des aspects cruciaux de soins équitables.
INTRODUCTION
The South Asian (SA) population includes diverse individuals originating from India, Bhutan, Pakistan, Nepal, Sri Lanka, and Bangladesh [1–2]. The SA diaspora is a subgroup that migrated to the Caribbean, Africa, Europe, Canada, the Middle East, and other parts of Asia and the Pacific Islands [1]. In Canada, the South Asian population reached 2.5 million in 2021 and is projected to increase to 5 million by 2041 [3–4]. The majority of South Asians reside in Toronto, Ontario, and Vancouver, British Columbia [5]. This population is disproportionately impacted by chronic diseases compared to their white counterparts (referring to those with European ancestry) [6–13], with SA adults having an 8.1 times higher prevalence of developing type 2 diabetes (herein referred to as diabetes) [8]. The latter exacerbates the prevalence of cardiovascular disease (CVD) [9–17].
Majority of the literature on SAs attribute the higher rates of diabetes and CVD to biomedical and behavioural risk factors [18]. Studies report SAs in Canada are more susceptible to diabetes due to their fetal programming [18], have a higher amount of visceral fat and fatty acids, lower HDL-cholesterol levels, and greater insulin resistance compared to whites [12, 18]. They also state SAs engage in less physical activity, have a high-caloric, fat diet, and low fibre intake [12, 18], which is postulated to occur through acculturation in Westernized countries [19–20]. Thus, diet and physical activity are often seen as modifiable risk factors for diabetes and CVD [2, 21–27]. However, these studies illustrate a white normative and pathologizing perspective on diet when making comparisons to other cultures [28–31]. This ignores the broader societal context and creates a discordance with nutrition recommendations in Canada [28, 32]. The individualistic focus disregards how chronic disease is influenced by the social determinants of health (SDH); the interplay of social, economic, and cultural aspects that affect an individual’s or population’s health status, which creates a circumstantial disadvantage for certain groups [33–37]. Current research suggests that the Social Ecological Model (SEM) is commonly utilized to map SDH (Figure 1). This model serves as a guiding framework to determine the causes of public health nutrition issues and to propose strategies for change [38–41, 46]. A key SDH for SAs and their chronic disease risk is racism [15, 35–37, 42]. SAs and other ethno-racial groups are met with white normativity in societal structures, including in nutrition care [28, 31, 35, 47].
Figure 1.
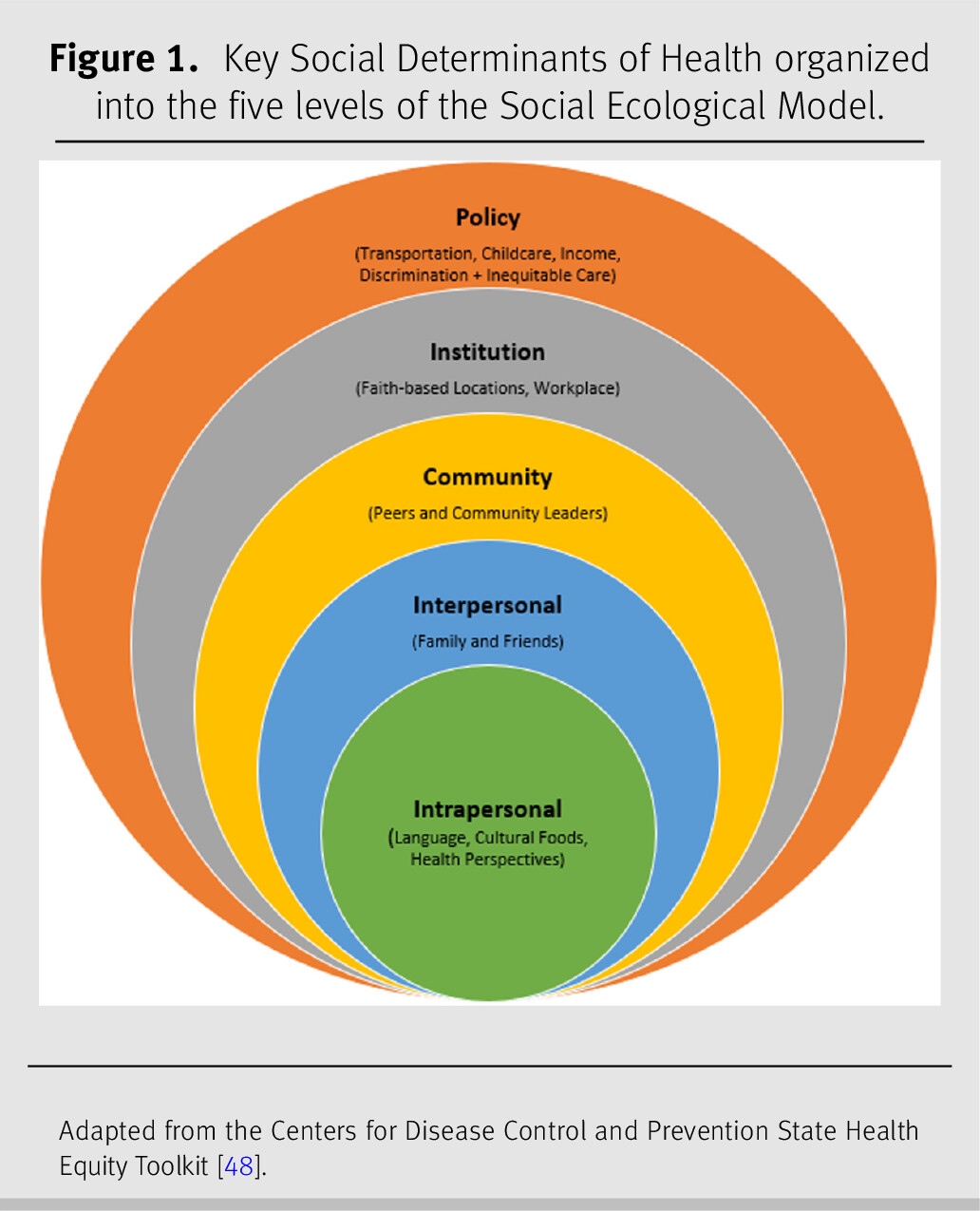
Figure 1. Key Social Determinants of Health organized into the five levels of the Social Ecological Model.
Adapted from the Centers for Disease Control and Prevention State Health Equity Toolkit [48].
There is limited literature supporting the influence of the SDH in nutrition care interventions for SAs, which ignores health inequities in this population. The aim of this narrative review [43–45] was to explore SDH in nutrition care interventions for diabetes and CVD in the SA diaspora residing in Canada, and to propose equity-informed recommendations for dietitians working with this population.
METHODS
Search strategy
For this narrative review, MEDLINE, CINAHL, and Scopus databases were searched in November 2021, using the following keywords: “nutrition education”, “nutrition counsel*”, “nutrition intervention*”, “family care”, “peer program”, “Bangladesh”, “India”, “Nepal”, “Pakistan”, “Sri Lanka”, “Bhutan”, “South Asia”, “Canada”, “culturally sensitive”, “culturally appropriate”, and “cultural safety”. Selection criteria included peer-reviewed journal articles that focused on SA adults residing in Canada with ancestral origins from Nepal, Bhutan, Pakistan, Bangladesh, India, or Sri Lanka, and nutrition interventions for SAs with type 2 diabetes and/or CVD. Articles were excluded if they included SAs residing outside of Canada or SAs with type 1 diabetes; if they were conferences or poster abstracts, letters, commentaries, editorials, and presentations; written in a language other than English; and were published before the year 2000 (previous 20 years to reflect the increase in diversity of SAs in Canada).
Data collection and synthesis
Two authors (SB and CB) screened articles by title and abstract. Descriptive phenomenology was used to chart key study information for studies meeting the eligibility criteria. The analysts (SB and CB) applied thematic analysis to independently identify relevant SDH in the articles and grouped them into the five SEM levels (Figure 1) [41, 46–48]. Analysts then compared their categorization, and disagreements were resolved by consensus.
RESULTS
The search generated a total of 957 articles, and fourteen articles met the eligibility criteria and were included in the final analysis (see Supplementary Figure1 for PRISMA Flow Diagram). The Supplemental Table summarizes key characteristics of the final studies. Included articles were published between 2009 and 2021 and had a sample size ranging from 9 to 184 participants. The majority (12/14 (86%)) were qualitative studies with semi-structured interviews and focus groups being the most common data collection method. Eleven (79%) focused on diabetes and three (21%) on CVD. The reviewed articles revealed several SDH that demonstrate how the individual is interconnected with different parts of society and how these interactions influence health [38, 47]. These SDH highlight how dietitians can improve nutrition care for SAs with diabetes and CVD in Canada. Table 1 includes a summary of the key findings.
Table 1.
Intrapersonal
Intrapersonal factors encompass an individual’s knowledge, attitudes, and beliefs [41]. Several studies in this review identified language, cultural foods, and health perspectives as central to an individual’s well-being. Language is a primary SDH for the SA diaspora [18]. In initial diabetes appointments, SAs report experiencing anxiety due to language barriers; with the fear of misunderstanding their practitioner’s recommendations and not being understood themselves [49–50]. When SA clients and dietitians spoke the same language, it increased the client’s engagement and comfort level in education sessions [51–53]. Resources in both English and the clients’ primary language were also beneficial to support understanding of nutrition management for diabetes and CVD [51, 54].
Moreover, cultural foods form an integral part of nutrition care [32, 55–56]. Studies indicated that SAs believed their cultural foods were a barrier to change [32, 53, 57–58]. Clients often were not given culturally appropriate diabetes education, and felt obliged to convert Western recipes into their respective cultures, and educate the dietitian [57]. In contrast, dietitians who considered their clients’ culture, increased their own awareness of culturally appropriate resources, and sought advice on cultural influences from colleagues which improved client care [58].
With common educational resources and their cultural adaptability, Mian and Brauer [51] found that clients suggested alternatives to the plate method, such as the thali; food served in small bowls on a round tray, and a more accurate measurement tool, such as a katori; a standard size metal bowl (approximately 150 ml). Education tools should also include visual representations of SA foods [51]. Although these findings are not universal across SAs, it is the dietitian’s role to inquire further about clients’ cultural foods when providing education [58].
Lastly, among health perspectives, a belief for some SAs is the notion of “cure vs. control”; that diabetes could be cured when glycemic control is achieved, thus leading to ceasing diabetes treatment and management [51]. Likewise, cultural views on using specific foods for diabetes management via phytotherapy, such as bitter melon, reduced clients’ adherence to medication [51, 57]. Additionally, faith and spirituality were important for some SAs post-myocardial infarction (MI), as they reported it being as or more significant than Western health care; it was how they understood and coped with accepting their condition [59]. Similarly, among older generations, there may be distrust in Western medicine and preference for Ayurvedic medicines [49]. Religious fasting is a key component for some Muslim and Hindu clients, with differences between and within these groups [51]. Community members described how healthcare providers focused on the negative impacts of fasting [60]. Culturally appropriate guidelines, created through practitioner–client collaboration, should focus on maintaining health while fasting (e.g., consider the amount and timing of foods consumed) [51, 54, 60].
Interpersonal
The interpersonal level refers to an individual’s family and friends and their influence on an individual’s dietary patterns, behaviour, and lived experiences [41]. Family was a key source of diabetes-related information for SAs, which decreased their likelihood of utilizing dietitian services [50]. For instance, SAs with gestational diabetes highly valued family knowledge, especially generational knowledge from elders (e.g., mother, mother-in-law, or grandmother) and sisters [58]. They often sought emotional and physical support from family members who already provided nutrition advice during pregnancy [57]. Additionally, SAs stated that a primary challenge in implementing dietary changes at home was that food was made for the entire family, and meal preparers needed to assist with implementing dietary changes [52, 59]. Family was described as an “externality” that should be included in diabetes education and management for SAs [52]. For example, when dietitians included a family member in diabetes appointments, it increased client adoption of dietary recommendations [51]. Family is also a facilitator for cardiac rehabilitation participation as they were found to be major social supports, through promoting client attendance and attending sessions with clients [61].
Moreover, collectivistic cultural norms for SAs during social gatherings with family and friends were a challenge, as they had to balance dietary changes for diabetes or CVD [51–52, 59]. As traditional foods were prepared with specific ingredients [58], clients perceived that foods high in sugar and fat were readily available and socially encouraged, and it was considered culturally impolite to refuse these meals [59]. Furthermore, SAs with gestational diabetes found it challenging to consider dietary changes and food preferences while preparing meals [58].
Community
The community level encompasses an individual’s secondary social networks [41]. For SAs, community members provide social support and nutrition advice [50, 58, 60–62]. When fasting during Ramadan, informal peer counseling provided by current Muslim clients with diabetes to new clients was more effective than patient education provided by dietitians [60]. Patients learned they were allowed to check blood sugars or break their fast if hypoglycemic [60]. Dahal and colleagues [49] also emphasize that a trusted community member is key in providing diabetes education and navigating services for SAs. A community leader was seen as a knowledge broker that bridged the healthcare system, and there was also more comfort in speaking with those that had similar cultural experiences [49]. A diabetes education and support program that trained peer leaders (with diabetes or who were diabetes caregivers) to provide behavioural and emotional support to SAs found that this improved diabetes distress levels [62]. However, clients suggested that aside from social support, it was equally important for peers to be knowledgeable about nutrition recommendations for diabetes [62].
Institution
The institution level highlights how organizations influence the individual [41]. One article reported that places of worship, such as temples, had limited opportunity for individuals to specify how or what food was prepared and served, since food practices are steeped in traditions [59]. Avoiding the dining area at temples was not appropriate, as it led to decreased socialization and potential isolation [52]. Although Tang and colleagues [62] agreed that faith-based locations provide social support to SAs, they noted it was not appropriate to deliver lifestyle modification interventions due to the availability of foods higher in fat, sugar, and salt. However, the authors’ [62] interpretation of foods offered at SA faith-based locations stigmatizes SA foods as “unhealthy” [39, 63–64]. Religious institutions are community hubs and prime locations for promoting services and offering peer support [52, 59, 61–62].
Additionally, employers were a barrier to accessing care for SAs. A few studies found the inability to take time off work to attend diabetes or cardiac education sessions was connected to financial limitations [51, 61]. To mediate this issue, Banerjee and colleagues [58] found that cardiac rehab programs offering evening sessions were more convenient, and preferred over other timings or nearby locations. This indicates that dietitians must be flexible in timing sessions to accommodate those clients with stricter work policies [51, 61].
Policy
The SEM’s final section focuses on social structures and systems that influence policy-level decisions, which in turn impact individual health [44, 45, 41]. Limited access to dietitian services due to inconvenient locations [51] or transportation needs [50, 53, 61] was identified as a barrier to diabetes and cardiac care. Childcare issues [50] and additional costs not covered by Ontario’s health insurance or other insurance providers were also of concern among SAs seeking diabetes care [50, 65]. Gucciardi and colleagues [66] reported that the cost of lancets and strips for diabetes discouraged daily self-monitoring among SAs, which had an adverse impact on goals for dietary management. Furthermore, the cost of eating a nutritious diet was a key barrier in Toronto for those in the South Asian Diabetes Prevention Program [53], and was an important predictor of diabetes self-management [65]. This suggests the need to address food insecurity among this population. Consequently, precarious employment and having a low income was more common among recent SA immigrants compared to non-racialized Canadian-born clients [50]. Although only one of the articles found that SAs experienced discriminatory and inequitable treatment by healthcare providers, this is a significant determinant for adopting diabetes self-management behaviours, such as eating a nutritious diet [65].
DISCUSSION
This is the first narrative review to utilize the SEM as a guiding framework to highlight the role of the SDH in nutrition care for SAs with diabetes and CVD in Canada. The SEM can encourage dietitians to address the SDH in their practice [33–34, 38]. The following SDH were identified in this review: language, cultural foods, health perspectives, family and friends, peers and community leaders, faith-based locations and workplaces, transportation, childcare, income, and, discrimination and inequitable care.
Studies in other countries on SAs have also demonstrated the SDH found in this review. A systematic review identified native language use, culturally specific resources, and family involvement as primary SDH for diabetes management [64]. As well, dietary changes for CVD management in SAs were difficult to maintain unless there was family support [67]. SAs perceived advice from peers as familiar and meaningful, while advice from clinicians was unfamiliar and devoid of cultural meaning [68–69]. Another study identified that dietary interventions to prevent diabetes in SAs, tend to be extrapolated from evidence found from non-SAs, and align with guidelines not developed for them [70]. Evidently, the need for co-created community-level interventions for SAs spans across different countries [64, 67–70].
Furthermore, workplaces were identified as a barrier for dietary change as many SAs report struggling financially [51, 61]. SA taxi drivers stated that financially supporting their families was a priority when deciding between attending a healthcare appointment and working; causing them to decide between health or earning an income [71]. This reflects the systemic issue of working a lower-wage and precarious job that lacks both work flexibility and income security [72–73]. The intersection between nutrition care and income is also evident through the prevalence of food insecurity (FI) [72–73]. Although only a few studies in this review discussed FI [53, 65], the prevalence of FI among SAs is high [18, 72, 74]. SAs account for 15.7% of FI households in Canada compared to 13.2% for white households [72]. Racialized and low-income groups are more likely to experience FI [72–75], resulting in poorer health [75–76], and a higher risk for diabetes and CVD-related complications [72, 77–81]. A study discussed service provider perspectives on two SDH, employment and income, for diabetes management in SAs [82]. It emphasized that racism impacts access to equitable employment, which further perpetuates income insecurity for SAs [83]. Racialized income inequality, along with structural barriers to education attainment, contribute to the experience of FI for SAs [68, 80–84]. A multi-level policy approach targeting systemic racism in education and employment can ultimately improve the health of the SA diaspora in Canada [72, 82].
Culture was an underlying theme in this review, as every culture has food-related values and beliefs [18, 88]. SAs value community and the need to preserve culture through traditional foods [18]. This ties directly into their well-being and how they interpret nutrition advice from healthcare providers [18]. The SDH in this review highlights the current status of Canadian dietitians’ cultural awareness, sensitivity, and competence when working with SAs. Providing culturally appropriate care encompasses awareness, acknowledgement, recognition, and respect around the differences between and within cultures [89]. Cultural competence focuses on the practitioners’ attainment of skills, knowledge, and attitudes to work respectfully with all cultural groups [89]. However, dietitians must foster cultural humility and safety to provide inclusive and equitable care to SAs [89]. Cultural humility is a lifelong process of self-reflection and accountability, allowing clinicians to acknowledge their biases, stereotypes, and prejudices [89]. Cultural safety takes a strength-based approach to culture in care; it considers the social, political, and historical context of care, and requires clinicians to practice cultural humility; and is only determined by the individual and their community [89].
Limitations
This review excluded SAs that originated from countries outside of SA, such as the Caribbean or Africa, as they may be considered a subgroup of the SA diaspora [1]. As well, SAs are discussed as a homogenous group in order to develop a general discourse [90] on SDH for nutrition care in this diaspora. However, it is important to recognize the diversity within SA communities, including differences in migration histories [90] and varying definitions of “healthy eating” [63, 91]. Future research should focus on discovering community-specific SDH for nutrition care.
Moreover, SAs in hospital settings were excluded, as dietary recommendations vary significantly between inpatient and outpatient care. Also, this review did not group findings based on immigrant status, which is a SDH that affects one’s ability to navigate a new environment [92–94]. Further investigation should explore this SDH in nutrition care for SAs.
Furthermore, this is not a systematic review, and therefore may lack the comprehensive and systematic nature of searching in all available databases, and did not include an assessment of study quality and certainty of the evidence. Nevertheless, narrative reviews provide a more focused understanding on a specific topic [45]. Lastly, the majority of literature found focuses on health behaviour change and disregards systemic inequities, such as classism and racism. Further research should assess these facets to highlight their pivotal role in nutrition care.
Recommendations
The following are equity-informed recommendations for dietitians working with SAs in Canada.
•
Include family in client sessions [51–52, 58–59, 61], create collaborative, community-driven nutrition interventions [94–95] (e.g., through informal peer counseling, peer groups, or designated community leaders) [49, 58, 60–62] and utilize faith-based locations as community hubs for disseminating education [53, 59, 61–62].
•
•
•
•
RELEVANCE TO PRACTICE
As Registered Dietitians, the SDH identified in this review present avenues for improving nutrition care for SAs with diabetes and CVD in Canada. These SDH reflect dietitians’ current cultural awareness, sensitivity, and competence when working with this population. However, the SEM as a guiding framework has highlighted that dietitians should focus on the SDH and implement strategies that consider cultural humility and safety. These equity-informed recommendations are a starting point for dietitians to improve their practice. As the SA population increases in Canada, dietitians must be prepared to utilize their clients’ strengths to provide the highest level of care.
Source(s) of financial support
There are no funding partners for this project, and none of the organizations had any role in the project design, analyses, interpretation of data, or writing of the manuscript.
Acknowledgements
None.
Footnote
1
Supplementary data are available with the article through the journal Web site at Supplementary Material.
Conflicts of interest: The authors declare that there are no competing interests.
Author contributions: SB and CB reviewed the data, completed the analysis, and wrote the manuscript. ATB and AM conceptualized the study and supervised the project. All authors have critically reviewed the results, revised this manuscript, and have approved the final manuscript.
REFERENCES
1
South Asian Americans Leading Together. Community resource guide: A demographic snapshot of South Asians in the United States; c2015 [cited 2023 Mar 17]. Available from: https://saalt.org/wp-content/uploads/2016/01/Demographic-Snapshot-updated_Dec-2015.pdf
2
Islam F, Khanlou N, and Tamim H. South Asian populations in Canada: migration and mental health. BMC Psychiatry. 2014;14:154.
3
Statistics Canada. Focus on geography studies, 2021 Census of population of Canada; c2022 [cited 2024 Jan 20]. Available from: https://www12.statcan.gc.ca/census-recensement/2021/as-sa/fogs-spg/page.cfm?topic=10&lang=E&dguid=2021A000011124#
4
Statistics Canada. Asian Heritage Month; c2023 [cited 2024 Jan 20]. Available from: https://www.statcan.gc.ca/o1/en/plus/3575-asian-heritage-month
5
Statistics Canada. The Canadian Census: A rich portrait of Canada’s Religious and ethnocultural diversity; c2022 [cited 2024 Jan 20]. Available from: https://www150.statcan.gc.ca/n1/daily-quotidien/221026/dq221026b-eng.htm
6
Peel Public Health. Diabetes Atlas for the Region of Peel; c2014 [cited 2023 Mar 17]. Available from: https://www.peelregion.ca/health/resources/diabetes-atlas/full-report.pdf
7
Statistics Canada. 2016 Census: Data products, 2016 Census profile; c2017 [cited 2023 Mar 17]. Available from: https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/prof/index.cfm?Lang=E.
8
Diabetes Canada. Diabetes in Canada. Toronto (ON): Diabetes Canada; c2022 [cited 2022 Mar 17]. Available from: https://www.diabetes.ca/DiabetesCanadaWebsite/media/Advocacy-and-Policy/Backgrounder/2022_Backgrounder_Canada_English_1.pdf
9
Diabetes Canada. Diabetes in Canada: Facts and figures from a public health perspective. Toronto (ON): Diabetes Canada; c2020 [cited 2022 Mar 17]. Available from: https://www.diabetes.ca/DiabetesCanadaWebsite/media/Advocacy-and-Policy/Backgrounder/2020_Backgrounder_Canada_English_FINAL.pdf
10
Forouhi NG and Sattar N. CVD risk factors and ethnicity—a homogeneous relationship?. Atheroscler Suppl. 2006 Apr 1;7(1):11–9.
11
Nestel S. Colour coded health care: The impact of race and racism on Canadians’ health. Toronto, ON: Wellesley Institute; c2012 [cited 2023 Mar 18]. Available from: http://www.wellesleyinstitute.com/health-care/colour-coded-health-care-the-impact-of-race-and-racism-on-canadians-health/
12
Rana A, de Souza RJ, Kandasamy S, Lear SA, and Anand SS. Cardiovascular risk among South Asians living in Canada: a systematic review meta-analysis. CMAJ Open. 2014 Sep 22;2(3):E183–E191.
13
Veenstra G and Patterson AC. South Asian-white health inequalities in Canada: intersections with gender and immigrant status. Ethn Health. 2016 Aug;21(6):639–48.
14
Vahabi M and Damba C. A feasibility study of a culturally and gender-specific dance to promote physical activity for South Asian immigrant women in the Greater Toronto Area. Women’s Health Issues. 2015 Jan-Feb;25(1):79–87.
15
Fraser Health Authority. South Asian Health Report; c2015 [cited 2023 Mar 18]. Available from: http://www.fraserhealth.ca/about-us/health-reports/
16
Huang D, Refaat M, Mohammedi K, Jayyousi A, Al Suwaidi J, and Abi Khalil C. Macrovascular complications in patients with diabetes and prediabetes. Biomed Res Int. 2017.
17
Stone JA, Houlden RL, Lin P, Udell JA, Verma S. Cardiovascular Protection in People With Diabetes. Diabetes Canada; c2023 [cited 2023 Mar 18]. Retrieved from https://www.diabetes.ca/health-care-providers/clinical-practice-guidelines/chapter-23#panel-tab_FullText.
18
Nallathamby, S. The social determinants of health related to the increased prevalence and risk of diabetes among South Asians in Canada [unpublished manuscript]. 2021. Available from: https://ir.library.dc-uoit.ca/bitstream/10155/1404/1/Nallathamby_Shabithalini.pdf
19
Lesser IA, Gasevic D, and Lear SA. The association between acculturation and dietary patterns of South Asian immigrants. PloS One. 2014 Feb 18;9(2):e88495.
20
Sanou D, O’Reilly E, Ngnie-Teta I, Batal M, Mondain N, Andrew C, et al. Acculturation and nutritional health of immigrants in Canada: a scoping review. J Immigr Minor Health. 2014 Feb;16(1):24–34.
21
Heart and Stroke Foundation of Canada. Risk Factors you Cannot Change. Ottawa: Heart and Stroke; c2018 [cited 2023 Mar 18]. Available from: https://www.heartandstroke.ca/stroke/risk-and-prevention/risk-factors-you-cannot-change
22
Garduño Diaz SD and Khokhar S. South Asian dietary patterns and their association with risk factors for the metabolic syndrome. J Hum Nutr Diet. 2013 Apr;26(2):145–55.
23
Hu FB. Dietary pattern analysis: a new direction in nutritional epidemiology. Curr Opin Lipidol. 2002 Feb;13(1):3–9.
24
LeCroy MN and Stevens J. Dietary intake and habits of South Asian immigrants living in Western countries. Nutr Rev. 2017 Jun 1;75(6):391–404.
25
Misra A, Khurana L, Isharwal S, and Bhardwaj S. South Asian diets and insulin resistance. Br J Nutr. 2009 Feb;101(4):465–73.
26
Block G, Gillespie C, Rosenbaum EH, and Jenson C. A rapid food screener to assess fat and fruit and vegetable intake. Am J Prev Med. 2000 May;18(4):284–8.
27
Gadgil MD, Anderson CA, Kandula NR, and Kanaya AM. Dietary patterns are associated with metabolic risk factors in South Asians living in the United States. J Nutr. 2015 Jun 1;145(6):1211–7.
28
Anderson LC, Mah CL, and Sellen DW. Eating well with Canada’s food guide? Authoritative knowledge about food and health among newcomer mothers. Appetite. 2015;91:357–365.
29
Ray K. The ethnic restaurateur. Bloomsbury Publishing; 2016.
30
Morris M. Standard white: Dismantling white normativity. California Law Rev. 2016 Aug 1:949–78.
31
Burt K. The whiteness of the Mediterranean Diet: A historical, sociopolitical, and dietary analysis using Critical Race Theory. Crit Dietetics. 2021;5(2):41–52.
32
Wilson T and Shukla S. Pathways to revitalization of Indigenous food systems: Decolonizing diets through Indigenous-focused food guides. J Agric Food Syst Community. 2020 Jun 12;9(4):201–8.
33
Government of Canada. Social Determinants of Health and Health Inequities; c2022 [cited 2023 Mar 18]. Available from: https://www.canada.ca/en/public-health/services/health-promotion/population-health/what-determines-health.html
34
Raphael D. Social determinants of health: Canadian perspectives. Toronto: Canadian Scholars’ Press; 2016.
35
National Collaborating Centre for Determinants of Health. Let’s talk: Racism and health equity. Antigonish, NS: NCCDH, St. Francis Xavier University; 2018.
36
Keval H. Risky cultures to risky genes: The racialised discursive construction of south Asian genetic diabetes risk. New Genetics and Society. 2015;34(3):274–293.
37
Mahajan A, Banerjee AT, Ricupero M, Beales A, Lac J, Ajwani F, et al. Call to action to improve racial diversity in dietetics. Critical Dietetics. 2021;5(2):3–9.
38
Golden SD and Earp JA. Social ecological approaches to individuals and their contexts: twenty years of health education & behavior health promotion interventions. Health Educ Behav. 2012 Jun;39(3):364–72.
39
Sallis JF, Owen N, Fisher EB. Ecological models of health behavior. In: Glanz K, Rimer BK, Viswanath K, editors. Health behavior and health education: theory, research, and practice. 4th ed. San Francisco: Jossey-Bass; 2008. pp. 465–86.
40
Gregson J, Foerster SB, Orr R, Jones L, Benedict J, Clarke B, et al. System, environmental, and policy changes: using the social-ecological model as a framework for evaluating nutrition education and social marketing programs with low-income audiences. J Nutr Educ. 2001;33 Suppl 1:S4–15.
41
Robinson T. Applying the socio-ecological model to improving fruit and vegetable intake among low-income African Americans. J Community Health. 2008;33:395–406.
42
Ng E. Ethnic food practices, health, and cultural racism: Diabetes risk discourse among racialized immigrants in Canada. Canadian Food Studies/La Revue canadienne des études sur l’alimentation. 2023 Mar 13;10(1):33–40.
43
Kirkevold M. Integrative nursing research—an important strategy to further the development of nursing science and nursing practice. J Adv Nurs. 1997 May;25(5):977–984.
44
Mays N, Pope C, and Popay J. Systematically reviewing qualitative and quantitative evidence to inform management and policy-making in the health field. J Health Serv Res Policy. 2005 Jul;10 Suppl 1:6–20.
45
Green BN, Johnson CD, and Adams A. Writing narrative literature reviews for peer-reviewed journals: secrets of the trade. J Chiropr Med. 2006;5(3):101–117.
46
Caperon L, Arjyal A, KC P, Kuikel J, Newell J, Peters R, et al. Developing a socio-ecological model of dietary behaviour for people living with diabetes or high blood glucose levels in urban Nepal: A qualitative investigation. PloS One. 2019 Mar 28;14(3):e0214142.
47
Glanz K, Rimer BK, Viswanath K, editors. Health behavior and health education: theory, research, and practice. John Wiley & Sons; 2008.
48
Centers for Disease Control and Prevention. Health Equity Resource Toolkit for State Practitioners Addressing Obesity Disparities; c2017 [cited 2023 Mar 18]. Available from: https://www.cdc.gov/nccdphp/dnpao/health-equity/state-health-equity-toolkit/index.html
49
Dahal G, Qayyum A, Ferreyra M, Kassim H, and Pottie K. Immigrant community leaders identify four dimensions of trust for culturally appropriate diabetes education and care. J Immigr Minor Health. 2014 Oct;16(5):978–84.
50
Hyman I, Patychuk D, Zaidi Q, and Kljujic D. Self-management, health service use and information seeking for diabetes care among recent immigrants in Toronto. Chronic Dis Inj Can. 2012;33(1):32–7.
51
Mian SI and Brauer PM. Dietary education tools for South Asians with diabetes. Can J Diet Pract Res. 2009;70(1):28–35.
52
Uppal G, Sibbald SL, and Melling J. Exploring diabetes management amongst immigrant Sikhs in the Greater Toronto Area: a qualitative study. Ethn Health. 2016;21(6):551–563.
53
Van Draanen J, Shafique A, Farissi A, Wickramanayake D, Kuttaiya S, Oza S, et al. How to offer culturally relevant type 2 diabetes screening: lessons learned from the South Asian Diabetes Prevention Program. Can J Diabetes. 2014 Oct;38(5):329–33.
54
Jones CA, Mawani S, King KM, Allu SO, Smith M, Mohan S, et al. Tackling health literacy: adaptation of public hypertension educational materials for an Indo-Asian population in Canada. BMC Public Health. 2011 Jan 3;11:24.
55
Monterrosa EC, Frongillo EA, Drewnowski A, de Pee S, and Vandevijvere S. Sociocultural influences on food choices and implications for sustainable healthy diets. Food Nutr Bull. 2020 Jun;41(2_suppl):59S–73S.
56
Vincze L, Barnes K, Somerville M, Littlewood R, Atkins H, Rogany A, et al. Cultural adaptation of health interventions including a nutrition component in Indigenous peoples: a systematic scoping review. Int J Equity Health. 2021;20(1):125.
57
De Sequeira S, Halperin I, and Lipscombe LL. Culturally tailored resources for south Asian immigrant women with gestational diabetes: do they work and what’s missing? A qualitative study. Can J Diabetes. 2019 Oct;43(8):573–579.
58
Kandasamy S, Nguyen L, Desai D, Anand SS, Sherifali D, and de Souza RJ. Barriers to, and facilitators of, lifestyle changes to prevent gestational diabetes: an interpretive description of South Asian women and health-care providers living and working in southern Ontario, Canada. Can J Diabetes. 2021 Apr;45(2):144–154.
59
Galdas PM, Oliffe JL, Wong ST, Ratner PA, Johnson JL, and Kelly MT. Canadian Punjabi Sikh men’s experiences of lifestyle changes following myocardial infarction: cultural connections. Ethn Health. 2012;17(3):253–266.
60
Pathy R, Mills KE, Gazeley S, Ridgley A, and Kiran T. Health is a spiritual thing: perspectives of health care professionals and female Somali and Bangladeshi women on the health impacts of fasting during Ramadan. Ethn Health. 2011 Jan;16(1):43–56.
61
Banerjee AT, Grace SL, Thomas SG, and Faulkner G. Cultural factors facilitating cardiac rehabilitation participation among Canadian South Asians: a qualitative study. Heart Lung. 2010 Nov-Dec;39(6):494–503.
62
Tang TS, Sohal PS, and Garg AK. Rethinking peer support for diabetes in Vancouver’s South-Asian community: a feasibility study. Diabet Med. 2015 Aug;32(8):1077–1084.
63
Chapman GE, Ristovski-Slijepcevic S, and Beagan BL. Meanings of food, eating and health in Punjabi families living in Vancouver, Canada. Health Educ J. 2011;70(1):102–112.
64
Sohal T, Sohal P, King-Shier KM, and Khan NA. Barriers and facilitators for type-2 diabetes management in South Asians: a systematic review. PLoS One. 2015 Sep 2;10(9):e0136202.
65
Hyman I, Shakya Y, Jembere N, Gucciardi E, and Vissandjée B. Provider-and patient-related determinants of diabetes self-management among recent immigrants: Implications for systemic change. Can Fam Physician. 2017;63(2):e137–e144.
66
Gucciardi E, Fortugno M, Senchuk A, Beanlands H, McCay E, and Peel EE. Self-monitoring of blood glucose in Black Caribbean and South Asian Canadians with non-insulin treated Type 2 diabetes mellitus: a qualitative study of patients’ perspectives. BMC Endocr Disord. 2013;13(1):1–10.
67
Osokpo O and Riegel B. Cultural factors influencing self-care by persons with cardiovascular disease: an integrative review. Int J Nurs Stud. 2021;116:103383.
68
Grewal S, Bottorff JL, and Hilton BA. The influence of family on immigrant South Asian women’s health. J Fam Nurs. 2005;11(3):242–263.
69
Greenhalgh T, Clinch M, Afsar N, Choudhury Y, Sudra R, Campbell-Richards D, et al. Socio-cultural influences on the behaviour of South Asian women with diabetes in pregnancy: qualitative study using a multi-level theoretical approach. BMC Med. 2015;13(1):1–15.
70
Muilwijk M, Nicolaou M, Qureshi SA, Celis-Morales C, Gill JM, Sheikh A, et al. Dietary and physical activity recommendations to prevent type 2 diabetes in South Asian adults: A systematic review. Plos One. 2018 Jul;13(7):e0200681.
71
Gany FM, Gill PP, Ahmed A, Acharya S, and Leng J. “Every disease… man can get can start in this cab”: focus groups to identify south Asian taxi drivers’ knowledge, attitudes and beliefs about cardiovascular disease and its risks. J Immigr Minor Health. 2013 Oct;15:986–92.
72
Tarasuk V, Li T, Fafard St-Germain AA. Household food insecurity in Canada, 2021. Toronto: Research to identify policy options to reduce food insecurity (PROOF); c2022 [cited 2023 Mar 18]. Available from: https://proof.utoronto.ca/.
73
Tarasuk V, Mitchell A, Dachner N. Household food insecurity in Canada 2014. Toronto, ON: Research to identify policy options to reduce food insecurity (PROOF); c2016 [cited 2023 Mar 18]. Available from: http://proof.utoronto.ca
74
Becerra MB and Chawdhury V. Health disparities among south Asians: is food insecurity the missing link. Electronic Theses, Projects, and Dissertations 2018;3:2.
75
Block S, Galabuzi GE. Persistent inequality. Canadian Centre for Policy Alternatives; 2018.
76
Ramsahoi CE, Sonny SS, and Monk JM. Exploring Barriers to Food Security Among Immigrants: A Critical Role for Public Health Nutrition. Can J Diet Pract Res. 2022;83(2):68–74.
77
Che J and Chen J. Food insecurity in Canadian households. Health Rep. 2001;12(4):11–22.
78
Gucciardi E, Vogt JA, DeMelo M, and Stewart DE. Exploration of the relationship between household food insecurity and diabetes in Canada. Diabetes Care. 2009 Dec 1;32(12):2218–24.
79
Tait CA, L’Abbé MR, Smith PM, and Rosella LC. The association between food insecurity and incident type 2 diabetes in Canada: a population-based cohort study. PloS One. 2018 May 2;13(5):e0195962.
80
Vozoris NT and Tarasuk VS. Household food insufficiency is associated with poorer health. J Nutr. 2003 Jan;133(1):120–6.
81
Kirkpatrick SI and Tarasuk V. Food insecurity is associated with nutrient inadequacies among Canadian adults and adolescents. J Nutr. 2008 Mar;138(3):604–612.
82
D’Silva C, Hafleen N, Mansfield E, Martel S, Fierheller D, Banerjee A, et al. Service provider perspectives on exploring social determinants of health impacting type 2 diabetes management for South Asian adults in Peel region, Canada. Can J Diabetes. 2022;46(6):611–9.
83
Tarasuk V, Mitchell A. Household food insecurity in Canada, 2017-18. Toronto: Research to identify policy options to reduce food insecurity (PROOF); c2020 [cited 2023 Mar 18]. Available from: https://proof.utoronto.ca/
84
Stapleton J. The working poor in the Toronto region: A closer look at the increasing numbers. Metcalf Foundation; 2019.
85
Naomi L and Luann GG. Measuring economic exclusion for racialized minorities, immigrants and women in Canada: results from 2000 and 2010. J Poverty. 2018;22.
86
Tarasuk V, Emery H. Household food insecurity in Canada, Part 1: food, nutrition, and health in the context of pervasive material deprivation; c2022 [cited 2023 Mar 18]. Available from: https://cns-scn.ca/education-portal/view/household-food-insecurity-in-canada-part-1-food-nutrition-and-health-in-the-context-of-pervasive-material-deprivation
87
Tarasuk V. Household food insecurity in Canada, Part 2: public policy responses and solutions; c2022 [cited 2023 Mar 18]. Available from: https://cns-scn.ca/education-portal/view/household-food-insecurity-in-canada-part-2-public-policy-responses-and-solutions
88
Knibb-Lamouche J. Culture as a social determinant of health. Seattle, WA: Commissioned paper prepared for the Institute on Medicine, Roundtable on the Promotion of Health Equity and the Elimination of Health Disparities; 2012.
89
Curtis E, Jones R, Tipene-Leach D, Walker C, Loring B, Paine SJ, et al. Why cultural safety rather than cultural competency is required to achieve health equity: a literature review and recommended definition. Int J Equity Health. 2019;18(1):1–17.
90
Islam T, Selvaratnam I, Shan N. Building an effective South Asian health strategy in Ontario. In Proceedings of the 3rd annual health equity conference. Council of Agencies Serving South Asians (CASSA); 2013. pp. 1–14.
91
Ristovski-Slijepcevic S, Chapman GE, and Beagan BL. Engaging with healthy eating discourse (s): Ways of knowing about food and health in three ethnocultural groups in Canada. Appetite. 2008 Jan 1;50(1):167–78.
92
Castañeda H, Holmes SM, Madrigal DS, Young MED, Beyeler N, and Quesada J. Immigration as a social determinant of health. Annu Rev Public Health. 2015;36:375–392.
93
Gagnon M, Kansal N, Goel R, and Gastaldo D. Immigration status as the foundational determinant of health for people without status in Canada: A scoping review. J Immigr Minor Health. 2022;1–16.
94
Banerjee AT and Shah B. One size does not fit all: Diabetes prevalence among immigrants of the South Asian Diaspora. J Immigr Minor Health. 2021;23(4):653–658.
95
Hofrichter R, Bhatia R, editors. Tackling health inequities through public health practice: theory to action. Oxford University Press, USA; 2010.
96
Wiggins N and Pérez A. Using popular education with health promotion students in the USA. Health Promot Int. 2017 Aug 1;32(4):660–70.
97
Banerjee AT, Mahajan A, Mathur-Balendra A, Qureshi N, Teekah M, Yogaratnam S, et al. Impact of the South Asian Adolescent Diabetes Awareness Program (SAADAP) on diabetes knowledge, risk perception and health behaviour. Health Educ J. 2022;81(1):96–108.
98
Harper GW, Jadwin-Cakmak L, Cherenak E, and Wilson P. Critical consciousness-based HIV prevention interventions for black gay and bisexual male youth. Am J Sex Educ. 2019 Jan 2;14(1):109–33.
99
Odoms-Young AM. Examining the impact of structural racism on food insecurity: implications for addressing racial/ethnic disparities. Fam Community Health. 2018;41(Suppl 2 FOOD INSECURITY AND OBESITY):S3.
100
Public Health Agency of Canada. Addressing stigma towards a more inclusive health system The Chief Public Health Officer’s Report on the State of Public Health in Canada 2019; c2019 [cited 2023 Mar 18]. Available from: https://www.canada.ca/content/dam/phac-aspc/documents/corporate/publications/chief-public-health-officer-reports-state-public-health-canada/addressing-stigma-what-we-heard/stigma-eng.pdf
101
Weaver HN. Between a rock and a hard place: A trauma-informed approach to documenting the traumatic experiences of Tamil refugees. J Hum Rights Soc Work. 2016;1:120–130.
Supplementary Material
Information & Authors
Information
Published In

Canadian Journal of Dietetic Practice and Research
Volume 86 • Number 1 • March 2025
Pages: 462 - 470
Editor: Naomi Cahill
History
Version of record online: 17 January 2025
Copyright
© 2024.
Key Words
Mots-clés
Authors
Metrics & Citations
Metrics
Other Metrics
Citations
Cite As
SharminiBalakrishnanMPH, RD, CristinaBeneaMPH, RD, AnanyaBanerjeePhD, and AnishaMahajanPhD, MPH, RD. 2025. Exploring the Social Determinants of Health in Nutrition Care for South Asian Communities: A Narrative Review. Canadian Journal of Dietetic Practice and Research.
86(1): 462-470. https://doi.org/10.3148/cjdpr-2024-024
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
Cited by
1. Nourishing Individuals So Our Communities Can Flourish
View Options
View options
Login options
Check if you access through your login credentials or your institution to get full access on this article.
Subscribe
Click on the button below to subscribe to Canadian Journal of Dietetic Practice and Research