Informing Evidence-based Practice in Nutritional Genomics: An Educational Needs Assessment of Nutrition Care Providers in Canada
Publication: Canadian Journal of Dietetic Practice and Research
7 August 2024
Abstract
Purpose: To investigate why Canadian nutrition care providers choose, or not, to integrate nutritional genomics into practice, and to evaluate the nutritional genomics training/education experiences and needs of nutrition providers in Canada, while comparing those of dietitians to non-dietitians.
Methods: A cross-sectional online survey was distributed across Canada from June 2021 to April 2022.
Results: In total, 457 healthcare providers (HCPs) [n = 371 dietitians (81.2%)] met the inclusion criteria. The majority (n = 372; 82.1%) reported having no experience offering nutritional genomics to clients (n = 4 did not respond). Of the 81 respondents with experience (17.9%), the most common reason to integrate nutrigenetic testing into practice was the perception that clients would be more motivated to change their eating habits (70.4%), while the most common reason for not integrating such tests was the perception that the nutrigenetic testing process is too complicated (n = 313; 84.1%). Dietitians were more likely than non-dietitians to view existing scientific evidence as an important educational topic (p = 0.002). The most selected useful educational resource by all HCPs was clinical practice guidelines (n = 364; 85.4%).
Conclusions: Both dietitians and non-dietitians express a desire for greater nutritional genomics training/education; specific educational needs differ by type of HCP. Low implementation of nutrigenetic testing may be partly attributed to other identified barriers.
Résumé
Objectif. Explorer pourquoi les fournisseurs de soins nutritionnels canadiens choisissent, ou non, d’intégrer la génomique nutritionnelle à leur pratique, et évaluer les expériences et besoins de formation en lien avec la génomique nutritionnelle des fournisseurs de soins nutritionnels au Canada, tout en comparant ceux des diététistes à ceux des non-diététistes.
Méthodes. Une enquête transversale en ligne a été distribuée partout au Canada entre juin 2021 et avril 2022.
Résultats. Au total, 457 fournisseurs de soins de santé (FSS) (n = 371 diététistes [81,2 %]) répondaient aux critères d’inclusion. La majorité (n = 372; 82,1 %) a déclaré n’avoir jamais offert à des clients des soins incluant de la génomique nutritionnelle (n = 4 n’ont pas répondu). Chez les 81 répondants ayant offert ce type de soins (17,9 %), la raison la plus fréquente d’intégrer les tests nutrigénétiques à la pratique était la perception que les clients seraient plus motivés à changer leurs habitudes alimentaires (70,4 %). La raison la plus fréquente de ne pas en intégrer était la perception que le processus de tests nutrigénétiques est trop complexe (n = 313; 84,1 %). Les diététistes étaient plus susceptibles que les non-diététistes de considérer les preuves scientifiques existantes comme un important sujet de formation (p = 0,002). La ressource de formation utile la plus sélectionnée par l’ensemble des FSS était les lignes directrices de pratique clinique (n = 364; 85,4 %).
Conclusions. Tant des diététistes que des non-diététistes aimeraient recevoir plus de formation sur la génomique nutritionnelle, et les besoins de formation diffèrent selon le type de FSS. Le faible recours aux tests nutrigénétiques pourrait être partiellement attribué à d’autres obstacles identifiés.
INTRODUCTION
Personalized nutrition (refer to Supplement A for a list of key terms and definitions) has been presented as “the most powerful antidote to chronic disease” [1]. In addition, registered dietitians (RDs) and other healthcare providers (HCPs), or non-RDs, perceive that personalized nutrition is “very important” within the field of nutrition [2]. Nutritional genomics (defined in Supplement A1), a key component of personalized nutrition, explores interactions between genetic variation, dietary intake, and subsequent health outcomes [3]. In Canada, regulatory bodies confirm that nutritional genomics is a component of dietetic practice [4, 5]. Consumers also view RDs as the best providers of nutrigenetic information and advice [6]. Additionally, the general public has expressed a substantial interest in personalized nutrition based on genetics [6, 7]. For instance, a Canadian study conducted in Quebec found that approximately 1 in 10 RDs had discussed nutritional genomics with their patients [8].
As rigorously trained and regulated HCPs, RDs are the most qualified nutrition care providers in Canada, but other HCPs also offer nutrition counselling and nutrigenetic tests (Supplement A) to patients. Concerns have been raised related to nutrition information communicated by unregulated nutrition care providers, including nutrigenetic information, and related to regulated HCPs such as medical doctors receiving insufficient nutrition education despite their extensive training [9–11]. Therefore, it is pertinent to understand the nutritional genomics education and training needs not only of RDs but also of other, non-RD nutrition care providers.
Despite the expectation that RDs and other HCPs play a key role in leading the incorporation of genetic information into nutrition care, research has consistently demonstrated that many lack knowledge, training, confidence, and competence in this field [2,12–19]. Nutritional genomics education is limited in undergraduate and graduate nutrition curriculum, and the quality and evidence-based nature of available training courses are variable [20,21]. In addition, the Academy of Nutrition and Dietetics’ current recommendations for dietitians wishing to develop expertise in nutritional genomics are quite broad and include elements such as staying on top of high-quality research in nutritional genomics and thinking critically about whether and how genetic testing should be translated into personalized interventions [22]. However, summarizing and grading scientific evidence are highly complex and time-consuming, and busy clinicians are unlikely to have the time and/or expertise to undertake such a task [23]. Systematic reviews and clinical practice guidelines (CPGs) would be useful to address this issue but are lacking in the field of nutritional genomics.
Studies have yet to thoroughly assess the experiences of nutrition care providers with nutritional genomics, and their specific educational and training needs [12–17,24]. Therefore, we sought to fill this gap. The objective of this study was to explore the reasons why nutrition care providers do or do not choose to integrate nutrigenetic testing into their practice and to assess the nutritional genomics training and education needs of nutrition care providers in Canada, while comparing the needs of RDs to those of non-RDs. The ultimate goal was to help guide evidence-based practice in nutritional genomics for RDs and non-RDs who are encountering or incorporating nutrigenetic testing in their practice by providing specific guidance for the development of evidence-based nutritional genomics training and educational materials.
METHODS
A cross-sectional, mixed methods study was conducted using a national online survey (Supplements B and C) made available in both English and French through the SurveyMonkey® platform.
Survey instrument
The survey (refer to Supplements B and C) contained questions that related directly to the study objectives. Its development was guided by existing literature. Gaps were identified in surveys of other studies exploring the education/training of HCPs in nutritional genomics, and questions were created to specifically address these gaps. In order to assess the face validity prior to data collection, a pilot test was conducted with 10 HCPs offering nutritional genomics in their practice and 10 not offering it in their practice. Revisions were then made to the survey based on feedback from HCPs. Data collection occurred from June 2021 to April 2022. This study was approved by the Ethics Committee of Université Laval.
Data collection
Participants were recruited through non-probability sampling. Survey links were emailed to nutrition-related organizations who helped with recruitment. In addition, participants were recruited through targeted social media advertisements (Facebook, Twitter) and through contacts within the researchers’ professional networks (convenience sampling) who were then asked to pass the survey link along to other nutrition HCPs (snowball sampling). To meet the inclusion criteria, participants had to provide nutrition information/advice to patients/clients within Canada. All participants provided informed consent before starting the survey and were given the opportunity to skip questions that they did not wish to answer throughout. As an incentive to participate, respondents were entered into a draw to win one of three $50 gift cards from grocery stores (should they have chosen to opt in). A sample size of n = 500 was determined to be the target based on previous studies [14,17,25]. Since this was an exploratory study with no specific primary outcome, a sample size calculation was not conducted.
Data analysis
Pooled and stratified statistical analyses were conducted. Participants were stratified based on RD compared to non-RD nutrition care providers. Descriptive statistics, chi-square and Fisher’s exact tests (when expected cell counts were <5) were conducted using SPSS version 28.0.1.1 (IBM, New York, USA, 2022). A p-value of 0.05 was used to determine statistical significance. Survey questions with open-ended responses (Questions 3–8, 10, 11, 13 in Supplements B and C) were analyzed qualitatively using inductive content analysis. This analysis was conducted by two researchers (JK and LMD), who first coded the qualitative data independently and proposed general themes for the open-ended responses. They then reviewed the independent themes and reached consensus through discussion, where necessary, to arrive at the final themes. A third researcher was not needed to resolve conflicts.
RESULTS
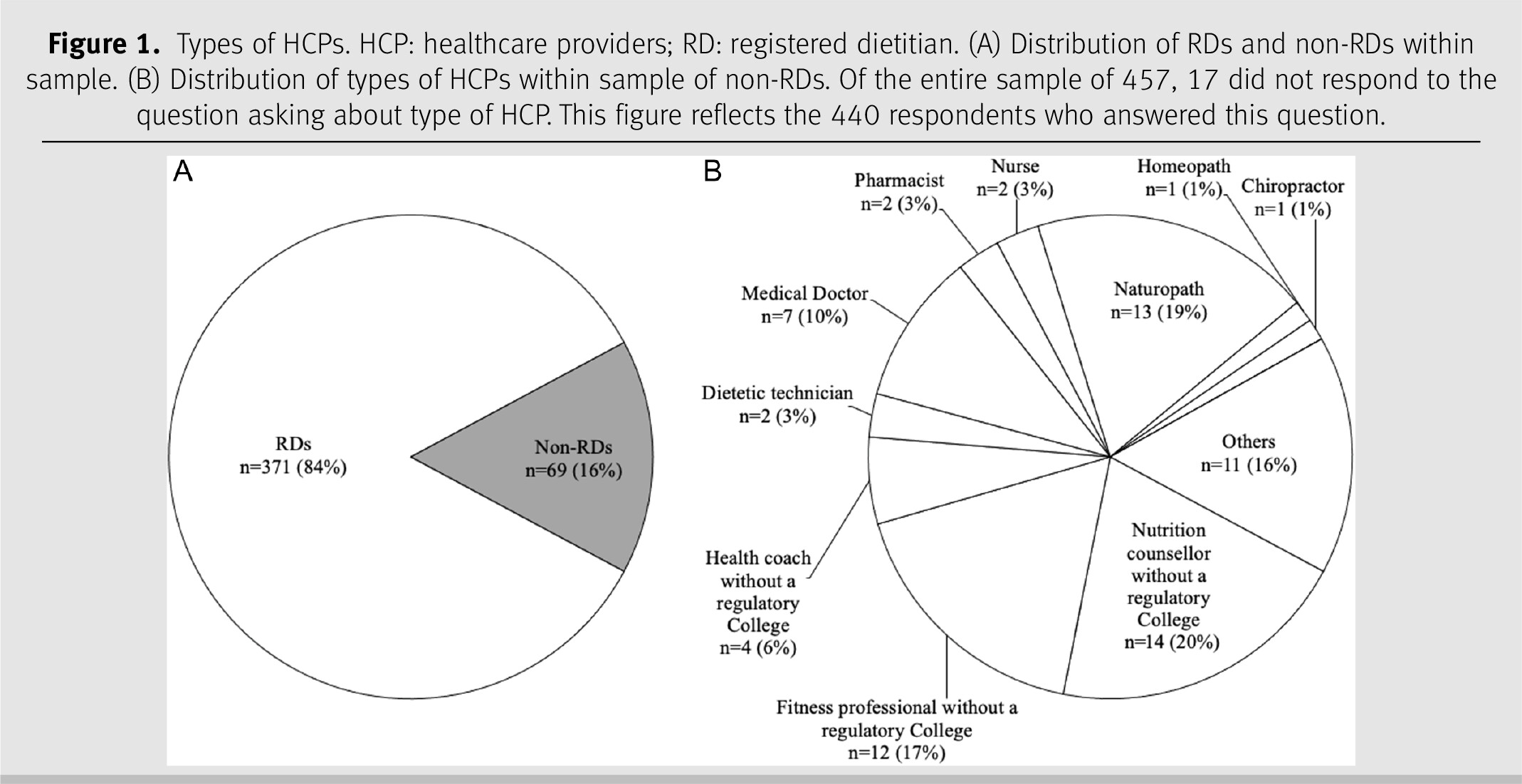
In total, 509 participants started the survey, resulting in a sample size of 457 participants who met the inclusion criteria and continued the survey. Response rates varied by questions; the specific sample size is indicated in the tables, figures, and text. Eighty-one respondents indicated that they had offered nutrigenetic testing to patients in their clinical practice either currently or in the past (17.9%); 372 respondents had never offered nutrigenetic testing to patients (82.1%) (missing data n = 4). The reasons why participants have or have not integrated nutrigenetic testing into their clinical practice are detailed in Table 1. Of the 81 respondents with clinical experience in nutrigenetics, 43 were RDs (53.1%) and 37 were non-RDs (45.7%) (missing data n = 1). Of the 372 respondents with no clinical experience in nutrigenetics, 327 were RDs (87.9%) and 31 were non-RDs (8.3%) (missing data n = 14). The types of HCPs among respondents are shown in Figure 1.
Table 1.
N.B. 5 participants did not answer this question.
Figure 1.
The level of education and training of the respondents in nutrition and nutrigenetics is depicted in Table 2. Overall, RDs had significantly higher levels of nutrition education than non-RDs (p < 0.001), with the exception of a significantly higher number of non-RD respondents with a doctorate degree (n = 4) compared to RDs (n = 2) (p < 0.001). In addition, significantly fewer RDs than non-RDs reported their primary source of nutritional genomics training/education as a college diploma (p = 0.007) and a master’s degree (p = 0.026). A total of 230 (50.3%) respondents had no training/education in nutritional genomics. Among the non-RDs with nutritional genomics training, most had obtained training/education through the nutrigenetic company who supplied the tests they sell to clients/patients. This was significantly less common in the RD group than in the non-RD group (p < 0.001). The qualitative analysis themes for participants responding “other” included obtaining additional nutritional genomics training/education from colleagues, university courses, and conferences.
Table 2.
*Results of chi-square or Fisher’s exact tests with statistical significance at p < 0.05 for RDs compared to non-RDs. NA: not applicable 1. Includes only respondents who indicated that they have obtained training/education in nutritional genomics; does not include 230 respondents who reported they had not obtained any additional training in this area.
The top three reasons why respondents reported integrating nutrigenetics into their clinical practice were (i) the perception that clients will be more motivated to change their diet with advice based on their genetics (70.4%; n = 57/81), (ii) the perception that their clients are interested in nutritional genomics/personalized nutrition (66.7%; n = 54/81), and (iii) the perception that their clients will have better health outcomes (58.0%; n = 47/81) (see Table 1). The qualitative analysis when participants selected “other” revealed the theme of perceived value to the patient. Furthermore, the main reason given by respondents for not implementing nutritional genomics in their clinical practice was (i) the belief that the implementation process is too complicated (84.1%; n = 313/372), (ii) the second most common reason given was that the respondent’s employer does not allow it (77.7%; n = 289/372), and (iii) while the third most popular response was the respondent’s personal lack of knowledge and understanding of nutritional genomics (64.2%; n = 239/372). In addition, key themes in the responses written under the “other” option included lack of relevance to their field of work, permission, lack of resources, and ethical considerations.
The topics considered most “useful” in the pooled sample included the practical application of nutritional genomics, its scientific validity, and its impact on health outcomes and dietary change. In this context, scientific validity refers to the quality and quantity of existing scientific evidence for a gene–diet association [26]. There were also significant differences between RDs and non-RDs in the perceived usefulness of these and other topics; for example, RDs were more likely (80.1%; n = 293/366) than non-RDs (62.5%; n = 40/64) to indicate that it would be beneficial to understand scientific validity in nutritional genomics (p = 0.002) (refer to Table 2). The applicability of nutritional genomics to specific areas of nutritional practice was a common theme in the open-ended responses regarding other priority training topics. In terms of most useful resources, significantly more RDs (91.5%; n = 332/363) perceived CPGs as a valuable resource compared to non-RDs (50.5%; n = 32/63; p < 0.001). In addition, a significantly greater proportion of RDs (RDs: 63.4%; n = 230/363 vs. non-RDs: 38.1%; n = 24/63; p < 0.001) perceived the value of position statements from regulatory bodies and nutrition organizations, as well as accredited comprehensive online courses compared to non-RDs (RDs: 65.6%; n = 238/363 vs. non-RDs: 55.6%; n = 35/63; p = 0.025). For those who selected “other,” the common theme identified was disease-specific guidelines. The topics deemed by RDs as priorities for future CPGs development were personalized nutrition for cardiometabolic disease prevention/management, followed by personalized nutrition for cancer prevention, and finally, macronutrients and their impact on body composition (see Supplementary Figure 2b). The lowest priority topics for RDs were genetically determined taste preferences and their impact on food/beverage intake, personalized nutrition for sports performance, and personalized nutrition for rare genetic diseases. In contrast, the highest priority for non-RDs was personalized nutrition for inflammation, followed by macronutrients and their impact on body composition, and micronutrient absorption/metabolism. Other priority topics for CPGs submitted by respondents in open-ended written responses were psychological/mental health, gastrointestinal health, and bone health.
DISCUSSION
This study assessed the educational needs and experiences of RDs and non-RD nutrition care providers in the field of nutritional genomics and evaluated differences between these two types of HCPs. It was observed that these HCPs are choosing to integrate nutritional genomics into their practice primarily because they perceive it is beneficial for their clients in a variety of ways. For example, respondents perceived that nutrigenetic testing could help motivate patients’ nutrition-related behaviour change, which is also supported by the findings of the most current systematic review of randomized controlled trials on this topic [27]. Client requests for genetic testing were also among the main reasons for implementation, reflecting the growing demand for personalized nutrition in Canada [6,7,28,29]. Nutrigenetic testing has been available in Canada for over a decade while sales have grown significantly since 2016 [30]. A recent analysis found that there are eight companies that offer nutrigenetic testing services to Canadians [9]; however, the market is constantly changing with some companies shutting down, and some new tests becoming available. Costs of these tests vary from $90 to $450 CAD depending on the provider [9]. While some provincial health plans cover genetic testing when a patient meets a pre-specified criteria, coverage remains limited. Instead, consumers typically pay out of pocket. This may explain why 29.8% of respondents reported they had not implemented nutrigenetic testing into their practice due to cost concerns.
Interestingly, respondents who did not integrate nutrigenetic testing into clinical practice indicated that they had not done so, because they considered the nutrigenetic testing process to be complicated. The process of nutrigenetic testing has recently been summarized elsewhere [9]. Manufacturers of nutrigenetic tests either sell them directly to the consumer or to HCPs who then sell them to their clients. In both cases, once the consumer has sent in their samples (typically from saliva or buccal swabs) to the nutrigenetic manufacturer, it is sent to a laboratory for DNA analysis. The results are either sent to the consumer for self-interpretation (along with supplementary information) or to their HCP. As such, the logistics of conducting nutrigenetic testing in clinical practice requires relatively little of the practitioner. They only need to collect a saliva or buccal cell sample from the client (if the company does not send the test kit directly to the patient/client). It is possible that the part of the process that is perceived as complicated is the interpretation of such results and their application in practice, which has been further detailed elsewhere [31]. Perhaps more complicated than the actual process of completing nutrigenetic testing in practice is obtaining the required knowledge of nutritional genomics to competently support clients to make dietary changes based on their results. Future research should explore this further, as the present study did not ask for elaboration on the exact component of the process that respondents perceived as complicated. Knowledge has proven to be a barrier for many, considering that a large proportion of respondents also claimed that the reason for not integrating nutritional genomics into clinical practice was a general lack of understanding of the topic. This is consistent with the current available literature that reports that RDs lack confidence and competency in nutritional genomics, which indicates a need for additional training and educational opportunities [2,12–18,19]. This lack of education is persistent in both Canada and other countries, where the implementation of nutrigenetic testing is also relatively new and thus highly variable [12,14]. In Canada however, several colleges such as the College of Dietitians of Alberta and the College of Dietitians of Ontario to name a few, along with Dietitians of Canada, have released statements in support of nutritional genomics falling within the scope of practice of RDs [4,9,32,33]. It should be noted that while one of the purposes was to explore facilitators and barriers towards nutrigenetic testing implementation, recommending for or against the use of nutrigenetic testing in practice is beyond the scope of this work. In addition, a large percentage of respondents (78%) reported that they had not implemented nutrigenetic testing in their practice because their employer did not allow it, while many were unaware of the existence of such tests or that they could offer such services. Improving our understanding of these perceived barriers would be a worthy topic for future research. In the meantime, the provision of educational resources could help raise awareness of this area of nutritional care among HCPs, as some respondents (n = 21) did not understand the significance of nutrigenetic testing.
In addition, low levels of formal nutrition education among non-RDs offering medical nutrition therapy (MNT) services are concerning. Dietitians must undergo rigorous training and are mandated and overseen by a regulatory body to ensure ethical and evidence-based practice, while other unregulated nutrition providers are not [34]. Our study found that the most commonly reported highest level of education for non-RDs was a certificate in nutrition from a private company. The development of educational resources in nutritional genomics must be designed with these varying levels of education in mind. Similarly, significantly more RDs than non-RDs perceived CPGs and position papers from regulatory bodies and nutrition organizations as valuable resources on nutritional genomics. Given that evidence-based decision-making is a required component of dietetic practice, it is not surprising that RDs perceived scientific validity as an important educational topic. In an effort to promote evidence-based practice for all nutrition providers, we must develop education/training resources that reach both RDs and non-RDs since presently both groups are permitted to practice MNT in Canada, including offering nutrigenetic testing [34]. A lack of evidence-based practice among non-RDs has recently been demonstrated in a study showing that unregulated, non-RDs are providing misleading and potentially harmful nutritional information to Canadians [35].
As nutrigenetics is already part of the clinical practice of some HCPs, there is an urgent need to develop CPGs so that clinicians can easily identify evidence-based gene–diet interactions. To our knowledge, there is only one existing CPG in nutritional genomics, related to genetically determined responsiveness to dietary omega-3 for alterations in lipids/lipoproteins [36]. Furthermore, there are only two systematic reviews with evidence grading in nutritional genomics (i.e. summarizing scientific validity) [36,37]. One of these reviews was used to guide the abovementioned omega-3 CPGs and identified two nutrigenetic associations with strong evidence, both related to genetic variation, omega-3 intake, and plasma triglyceride responsiveness [36]. Given that conducting systematic reviews and developing good practice guidelines (where appropriate) are resource intensive and that research in this area is rapidly evolving, it may be prudent to develop expert consensus statements. Dietitians in our study identified cardiometabolic disease prevention/management and personalized nutrition for cancer prevention as the first and second priority topics for future CPGs. The latter is a highly feasible topic for future CPGs given that a systematic review with evidence grading on this topic has already been completed recently [37]. This review demonstrated “moderately strong evidence (Grade BBB)” for the association between the 10p14 locus and elevated colorectal cancer risk when processed meat consumption is high [37]. In terms of clinical applications, these findings suggest that depending on genetic variation at the 10p14 locus, it may be particularly important for some patients to limit their processed meat consumption for colorectal cancer risk reduction.
More systematic reviews would also be helpful in informing the development of evidence-based educational resources, especially as scientific validity was highlighted as an important component of training on nutrigenomics by respondents. When establishing the levels of evidence for certain gene–diet interactions in future CPGs, a modified version of the framework proposed by Boffeta et al. has been recommended for use [26]. Partnerships with organizations such as Dietitians of Canada, Practice-Based Evidence in Nutrition (PEN), and dietetic curriculum developers could be useful in developing educational/training resources and increasing awareness of nutritional genomics among nutrition care providers.
As with all research, there are some limitations that exist in this study. Our questionnaire did not include questions on respondent demographics; therefore, we are unable to evaluate if our sample was representative of HCPs across Canada or describe personal factors that may have influenced responses such as the practice setting or number of genetic tests administered. In addition, the non-RD group was heterogeneous and included both regulated and non-regulated HCPs. The small numbers of the different types of non-RD HCPs limited our ability to conduct further subgroup analyses. Although the current results can only be generalized to dietitians and other nutritional care providers in Canada who work directly with patients, HCPs who do not work directly with patients are unlikely to encounter nutritional genomics in their practice and therefore may not be as willing to seek training in this area. Respondent bias is also a potential limitation of survey-based research [38]. Nutrition providers with a particular interest in nutritional genomics could have been more likely to respond to the survey. In addition, since survey questions could be skipped, some respondents chose to skip certain questions leading to different and sometimes smaller sample sizes for different questions. Due to this, it is possible that some statistically significant results may have been missed. Despite these limitations, this study provided a comprehensive and robust overview of the specific educational and training needs of various nutrition providers offering nutrition advice in Canada related to the increasingly popular science of nutritional genomics.
RELEVANCE TO PRACTICE
Ultimately, this research highlights (i) the need for CPGs covering the scientific validity (or lack thereof) for nutrigenetic interactions related to common health conditions such as cardiometabolic disease; in addition to (ii) the need for specific resources tailored for non-RD nutrition providers such as a comprehensive online course; and (iii) the requirements for greater education and training in nutritional genomics in order to enable RDs and non-RDs who provide nutrition information/advice with the skills necessary for implementing (if they choose to) evidence-based nutrigenetic testing in their practice. This study demonstrated that HCPs primarily embrace nutrigenetics in their practice to enhance client outcomes, with the main barrier to integration being the perceived complicated nature of the nutrigenetic process. By collecting data on HCPs’ current level of knowledge on this topic, their preferred method of learning, and their topics of interest, we are better able to target future interventions and education to encourage evidence-based nutrigenetic practices for all Canadians seeking personalized nutrition services.
Funding
A grant from the Canadian Foundation for Dietetic Research funded this research. JK received a CIHR Postdoctoral Fellowship. MCV is Canada Research Chair in Genomics Applied to Nutrition and Metabolic Health.
Conflict of interest
The authors declare that they have no competing interests.
Footnote
1
Supplementary data are available with the article at Supplementary Material.
REFERENCES
1
Newton RS, Blumberg JB, Reed DG, and Stroka MA. The American Nutrition Association®: Championing the science and practice of personalized nutrition. J Am Coll Nutr. 2020;39(1):1–4.
2
Kaufman-Shriqui V, Salem H, Boaz M, and Birk R. Knowledge and attitudes towards nutrigenetics: Findings from the 2019 Unified Forces Preventive Nutrition Conference (UFPN). Nutrients. 2020 Jan 27;12(2):335.
3
Sales NMR, Pelegrini PB, and Goersch MC. Nutrigenomics: Definitions and advances of this new science. J Nutr Metab. 2014;2014:1–6.
4
College of Dietitians of Alberta. Nutrigenomics in dietetic practice. College of Dietitians of Alberta Position Statement; 2015. p. 7.
5
Cohen D. Keeping pace with innovations in nutrition care. College of Dietitians of Ontario: Résumé; 2014. p. 4.
6
Nielsen DE, Shih S, and El-Sohemy A. Perceptions of genetic testing for personalized nutrition: a randomized trial of DNA-based dietary advice. J Nutrigenet Nutrigenom. 2014;7(2):94–104.
7
Stewart-Knox BJ, Bunting BP, Gilpin S, Parr HJ, Pinhão S, Strain JJ, et al. Attitudes toward genetic testing and personalised nutrition in a representative sample of European consumers. Br J Nutr. 2008 Sep 8;101(7):982–9.
8
Bouchard-Mercier A, Desroches S, Robitaille J, and Vohl M-C. Factors associated with the intention of registered dietitians to discuss nutrigenetics with their patients/clients. Can J Diet Pract Res. 2016;77(4):163–9.
9
Horne J, Gilliland J, Madill J, and Shelley J. A critical examination of legal and ethical considerations for nutrigenetic testing with recommendations for improving regulation in Canada: from science to consumer. J Law Biosci. 2020 Apr;7(1):1–20.
10
Gramlich LM, Olstad DL, Nasser R, Goonewardene L, Raman M, Innis S, Wicklum S, Duerksen D, Rashid M, Heyland D, Armstrong D, and Roy C. Medical students’ perceptions of nutrition education in Canadian universities. Appl Physiol Nutr Metab. 2010 Jun;35(3):336–43.
11
Collier R. Canadian medical students want more nutrition instruction. CMAJ. 2009 Aug 4;181(3-4):133–4.
12
Li SX, Collins J, Lawson S, Thomas J, Truby H, Whelan K, et al. A preliminary qualitative exploration of dietitians’ engagement with genetics and nutritional genomics: perspectives from international leaders. J Allied Health. 2014;43(4):221–8.
13
Cormier H, Tremblay BL, Paradis A-M, Garneau V, Desroches S, Robitaille J, et al. Nutrigenomics - perspectives from registered dietitians: a report from the Quebec-wide e consultation on nutrigenomics among registered dietitians. J Hum Nutr Diet. 2014 Aug;27(4):391–400.
14
Collins J, Bertrand B, Hayes V, Li SX, Thomas J, Truby H, et al. The application of genetics and nutritional genomics in practice: an international survey of knowledge, involvement and confidence among dietitians in the US, Australia and the UK. Genes Nutr. 2013 Nov;8(6):523–33.
15
Abrahams M, Frewer LJ, Bryant E, and Stewart-Knox B. Factors determining the integration of nutritional genomics into clinical practice by registered dietitians. Trends Food Sci Technol. 2017 Jan 1;59:139–47.
16
Wright ORL. Systematic review of knowledge, confidence and education in nutritional genomics for students and professionals in nutrition and dietetics. J Hum Nutr Diet. 2014 Jun;27(3):298–307.
17
Rosen R, Earthman C, Marquart L, and Reicks M. Continuing education needs of registered dietitians regarding nutrigenomics. J Am Diet Assoc. 2006 Aug 1;106(8):1242–5.
18
Lapham EV, Kozma C, Weiss JO, Benkendorf JL, and Wilson MA. The gap between practice and genetics education of health professionals: HuGEM survey results. Genet Med. 2000 Aug;2(4):226–31.
19
Whelan K, McCarthy S, and Pufulete M. Genetics and diet--gene interactions: involvement, confidence and knowledge of dietitians. Br J Nutr. 2008 Jan;99(1):23–8.
20
Collins J, Adamski MM, Twohig C, and Murgia C. Opportunities for training for nutritional professionals in nutritional genomics: What is out there?: Nutritional genomics professional development. Nutr Diet. 2018 Apr;75(2):206–18.
21
Horne J, Madill J, and O’Connor C. Nutrigenomics: an evident need for education in the field of dietetics. Can J Diet Pract Res. 2015 Aug;76(3).
22
Braakhuis A, Monnard CR, Ellis A, and Rozga M. Consensus Report of the Academy of Nutrition and Dietetics: Incorporating Genetic Testing into Nutrition Care. J Acad Nutr Diet. 2021 Mar;121(3):545–552.
23
Horne JR and Vohl M-C. Response to the consensus report of the academy of nutrition and dietetics: incorporating genetic testing into nutrition care. J Acad Nutr Diet. 2020;120(12):1959–1960.
24
Abrahams M, Frewer L J, Bryant E, and Stewart-Knox B. Perceptions and experiences of early-adopting registered dietitians in integrating nutrigenomics into practice. Br Food J, 2018 Apr; 120(4):763–776.
25
Mustapa MAC, Amin L, and Frewer LJ. Predictors of stakeholders’ intention to adopt nutrigenomics. Genes Nutr. 2020 Sep 22;15(1):16.
26
Keathley J, Garneau V, Zavala-Mora D, Heister RR, Gauthier E, Morin-Bernier J, Green R, and Vohl M-C (2021) A systematic review and recommendations around frameworks for evaluating scientific validity in nutritional genomics. Front. Nutr. 8:789215.
27
Jinnette R, Narita A, Manning B, McNaughton SA, Mathers JC, and Livingstone KM. Does personalized nutrition advice improve dietary intake in healthy adults? A systematic review of randomized controlled trials. Adv Nutr. 2021 Jun;12(3):657–669.
28
Vallée Marcotte B, Cormier H, Garneau V, Robitaille J, Desroches S, and Vohl MC. Current knowledge and interest of French Canadians regarding nutrigenetics. Genes Nutr. 2019 Feb 19;14:5.
29
Morin K. Knowledge and attitudes of Canadian consumers and health care professionals regarding nutritional genomics. OMICS. 2009 Feb;13(1):37–41.
30
Crow D. A new wave of genomics for all. Cell. 2019 Mar;177(1):5–7.
31
Horne JR, Nielsen DE, Madill J, Robitaille J, Vohl MC, and Mutch DM. Guiding global best practice in personalized nutrition based on genetics: The development of a nutrigenomics care map. J Acad Nutr Diet. 2022 Feb;122(2):259–269.
32
Dietitians of Canada. Nutrigenomics: Genetic testing for personalized nutrition [Internet]. Dietitians of Canada; 2023 [cited 2023 Apr 17]. Available from https://members.dietitians.ca/DCMember/LearnProduct?id=01tf4000003j6wPAAQ
33
Cohen D. Keeping pace with innovations in nutrition care [Internet]. College of Dietitians of Ontario; 2014 [cited 2023 Apr 17]. Available from: https://www.collegeofdietitians.org/resources/client-centred-services/client-centred/keeping-pace-with-innovations-in-nutrition-care-(2.aspx
34
Keathley JR, Arbour A, and Vohl MC. Towards a standardized definition of medical nutrition therapy and regulatory reform in Canada. Can J Diet Pract Res. 2022 Jun 1;83(2):75–80.
35
Toth J, O’connor C, Hartman B, Dworatzek P, and Horne J. “Detoxify or Die”: Qualitative assessments of Ontario nutritionists’ and dietitians’ blog posts related to detoxification diets. Can J Diet Pract Res. 2019 Sep 1;80(3):116–121.
36
Horne J, Desroches S, Garneau V, Vohl M-C. A systematic review and clinical practice guidelines for nutrigenomics, omega-3, plasma lipoproteins and lipids. PROSPERO 2020 CRD42020185087 [Internet]; 2020 [cited 2023 Apr 17]. Available from: https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=185087
37
Theodoratou E, Timofeeva M, Li X, Meng X, and Ioannidis JPA. Nature, nurture, and cancer risks: Genetic and nutritional contributions to cancer: Annu Rev of Nutr. 2017:37(1): 293–320.
38
Mazor KM, Clauser BE, Field T, Yood RA, and Gurwitz JH. A demonstration of the impact of response bias on the results of patient satisfaction surveys. Health Serv Res. 2002 Oct;37(5):1403–17.
Supplementary Material
File (cjdpr-2024-010suppla.docx)
- Download
- 57.41 KB
Information & Authors
Information
Published In

Canadian Journal of Dietetic Practice and Research
Volume 85 • Number 4 • December 2024
Pages: 379 - 387
Editor: Naomi Cahill
History
Version of record online: 7 August 2024
Copyright
© 2024.
Key Words
Mots-clés
Authors
Metrics & Citations
Metrics
Other Metrics
Citations
Cite As
PaulinaMorelliBASc, VéroniqueGarneauMSc, RD, LaurieMiville-DeschênesBSc, RD, JosianeMorin-BernierBSc, RD, Marie-ClaudeVohlPhD, SophieDesrochesPhD, RD, and JustineKeathleyPhD, RD. 2024. Informing Evidence-based Practice in Nutritional Genomics: An Educational Needs Assessment of Nutrition Care Providers in Canada. Canadian Journal of Dietetic Practice and Research.
85(4): 379-387. https://doi.org/10.3148/cjdpr-2024-010
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
There are no citations for this item
View Options
View options
Login options
Check if you access through your login credentials or your institution to get full access on this article.
Subscribe
Click on the button below to subscribe to Canadian Journal of Dietetic Practice and Research